





Bibliometric Analysis of Obesity and Heart Disease Research
From Numbers to Insights: Bibliometric Analysis of Obesity and Heart Disease Research Output
Sally Sonia Simmons¹˒², John Elvis Hagan Jr³˒⁴, Medina Srem-Sai⁵, Thomas Schack⁴
- Department of Social Policy, London School of Economics and Political Science, London, United Kingdom
- Institute of Demography, National Research University-Higher School of Economics, Moscow, Russia
- Department of Health, Physical Education & Recreation, College of Education Studies, University of Cape Coast, Ghana
- Neurocognition and Action Research Group-Biomechanics, Faculty of Psychology & Sport Sciences/CITEC, Bielefeld University, Germany
- Department of Health, Physical Education, Recreation and Sports, University of Education, P.O. Box 25, Winneba, Ghana
OPEN ACCESS
PUBLISHED: 31 August 2024
CITATION: Simmons, S.S., Hagan, J.E., et al., 2024. From Numbers to Insights: Bibliometric Analysis of Obesity and Heart Disease Research Output. Medical Research Archives, [online] 12(8).
https://doi.org/10.18103/mra.v12i8.5438
COPYRIGHT: © 2024 European Society of Medicine. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i8.5438
ISSN 2375-1924
Abstract
Despite significant research advancements, there remain important gaps in the understanding and directions for future investigations regarding obesity and heart disease. Therefore, this study examined the research output on obesity and heart disease across different countries and regions worldwide from 1970 to 2022. Using bibliometric analysis, a comprehensive dataset of 28,315 published articles related to obesity and heart disease was analysed. Specifically, the trends, patterns, recurring and spatial distribution of topics per the income level of countries and indices for measurement in obesity and heart disease research were analysed. A noticeable increase in research activity on obesity and heart disease was established across all regions globally. Notably, North America, Europe, and Central Asia exhibited a higher prevalence of research in these areas, while Sub-Saharan Africa and South Asia showed comparatively lower levels. The research encompassed a diverse range of themes, with a significant proportion of studies focused on obesity indices and comorbidities associated with these conditions. Other results revealed the identification of various anthropometric indices, biomarkers, and comorbidities from the examined studies. Body mass index, waist-to-hip ratio, waist circumference, hip circumference, fasting blood glucose, cholesterol, and lipoprotein levels emerged as recurring indices in the literature. Additionally, prevalent comorbidities associated with obesity and heart disease included diabetes, stroke, and metabolic syndrome. The findings can guide future research endeavours and public health interventions targeted at addressing the complex challenges posed by obesity and heart disease. This study underscores the global significance of obesity and heart disease as areas of scientific inquiry. Thus, this study serves as a clarion call for sustained and collaborative efforts, emphasising the pivotal role of ongoing research in forging a healthier and more informed global future.
Keywords
anthropometric indices, BMI, bibliometry, biomarkers, countries
List Abbreviations
- AU: Australia
- AT: Austria
- BD: Body density
- BE: Belgium
- BMR: Basal metabolic rate
- BR: Brazil
- BSS: Body surface area
- BV: Blood volume
- CA: Canada
- CC: Chest circumference
- CHR: Chest-to-hip ratio
- CL: Calf circumference
- CL: Chile
- CN: China
- DZ: Algeria
- EB: Elbow breadth
- GFD: Gluteofemoral fat mass
- DK: Denmark
- EG: Egypt
- EU: England
- FI: Finland
- FR: France
- NL: Netherlands
- HB: Head breadth
- HC: Hip circumference
- HHR: Hip-to-height ratio
- HICs: High-Income Countries
- KB: Knee breadth
- LBM: Lean body mass
- LMICs: Low- and Middle-Income Countries
- IN: India
- IE: Ireland
- JP: Japan
- MX: Mexico
- PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SE: Sweden
- SMM: Skeletal muscle mass
- STR: Standing height
- TC: Thigh circumference
- TCR: Thigh-to-calf ratio
- TL: Trunk length
- TR: Turkey
- US: USA
- WC: Waist circumference
- WCR: Waist-to-hip ratio
- WRC: Wrist circumference
- WHR: Waist-to-height ratio
- WHTHR: Waist-to-hip-to-thigh ratio
- WHTR: Waist-to-hip-to-trunk ratio
- WOS: Web of Science
- WTR: Waist-to-thigh ratio
Introduction
Navigating the intricate terrain of public health requires a keen understanding of the multifaceted challenges posed by prevalent health issues. In this dynamic landscape, obesity emerges as a significant risk factor, intricately linked to the development of hypertension, dyslipidaemia, insulin resistance, and inflammation—precursors that propel the progression of heart disease. Consequently, the rise in obesity rates has been accompanied by a parallel increase in the prevalence of heart disease. These health conditions are influenced by diverse factors and exert profound impacts across socioeconomic strata. Obesity, a complex health condition with far-reaching implications, is commonly assessed through anthropometric indices and biomarkers. Anthropometric measures, such as body mass index (BMI), waist-to-hip ratio (WHR) and waist circumference (WC) provide quantitative assessments of an individual’s body composition and fat distribution, whereas biomarkers like fasting blood glucose, cholesterol, and lipoprotein levels provide endoscopic assessment of the body’s composition.
While a plethora of studies have probed various facets of the intricate relationship between obesity and heart disease, a critical gap remains, as the structure of knowledge encompassing thematic and spatial patterns, recurring topics, and connections between different concepts related to obesity and heart disease, remain inadequately understood. Therefore, evaluating the structure and dynamics of scientific knowledge on this complex relationship is crucial and holds high value for a holistic understanding of the content and trends of research on obesity and heart diseases and informs the development of effective health policies and research strategies. This study employs a bibliometric analysis to discern pertinent publications worldwide regarding obesity and heart disease. Bibliometrics is defined as “the application of mathematical and statistical methods to books and other media of communication.” This methodology enables the comprehensive analysis of a substantial body of scientific literature within a particular research domain. Applying this approach to obesity and heart disease research provides a valuable means to scrutinise trends in published works over time, recurring areas of interest and topics, identify research gaps for future endeavours, explore innovative applications, highlight research significance, and pinpoint key references on a given theme.
This study provides a comprehensive review of the current literature on obesity and heart disease. By examining the trends, topics, geospatial contributions of studies on these conditions, the study uncovers and categorises dynamic or prevalent themes within the body of literature on obesity and heart disease. Besides, this comprehensive review is essential for directing future research efforts towards unexplored or underexplored facets of obesity and heart disease, contributing to a more comprehensive understanding of the content of existing information.
Materials and Methods
DATA SOURCE
Data for the study was retrieved from the Web of Science (WOS) from 1970-2022. WOS is a comprehensive research database and citation index that provides access to a vast collection of scholarly literature across various disciplines. Researchers, scientists, and scholars widely use WOS to search and retrieve academic articles, conference proceedings, and other research. Furthermore, the period from 1970 to 2022 witnessed significant lifestyle changes, medical advancements, and public health policies associated with diseases cardiovascular diseases. Consequently, studying this period allows for considering the effects of those shifts in livelihood to better understand the long-term trends and changes in obesity and heart disease epidemiology.
MEASUREMENTS
Web of Science (WOS) Data Extraction, Inclusion and Exclusion Criteria
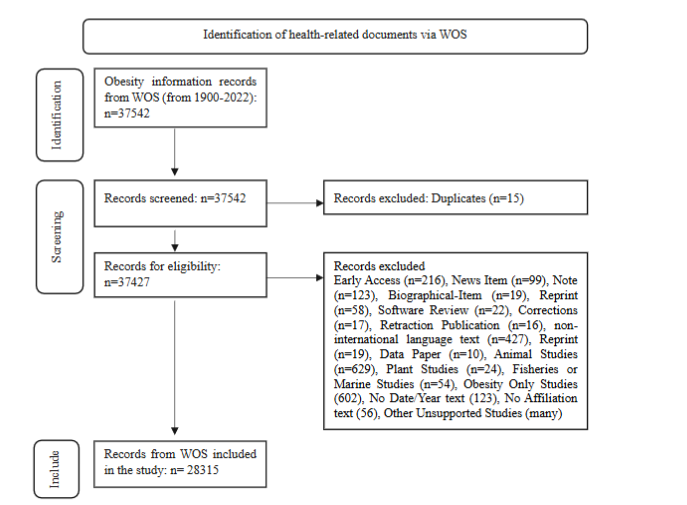
To review and synthesise the literature on obesity and heart disease, we utilised the preferred method for systematic reviews and meta-analyses (PRISMA) approach. This approach ensures a systematic and transparent process of gathering, evaluating, and synthesising relevant research findings in a rigorous and reproducible manner. Following the PRISMA guidelines, the goal was to present a comprehensive and reliable overview of the current evidence regarding the association between obesity and heart disease. Specifically, we utilised the PRISMA guidelines to identify studies that addressed both obesity and heart diseases. This approach was grounded in the recognised correlation between obesity and heart diseases, as highlighted by Powell-Wiley and colleagues. Consequently, there was an unrestricted title search using “obesity,” “obese,” “heart diseases,” “heart,” “disease,” “diseases,” “coronary heart disease,” “ischaemic heart disease,” “coronary disease,” “cardiovascular disease,” or “cardiac disease,” from the WOS database. The initial sample for the study consisted of 37,542 documents. To improve the quality and focus of the text, certain types of documents were excluded from the analysis, such as obesity only text, no affiliation and date texts, data papers, corrections, news items, reprints, software reviews, notes, early access articles, biographies, non-international language texts, and retractions. The main bibliometric information extracted from the retrieved texts included abstracts, affiliations, and the year of publication. Careful evaluation of the abstracts was conducted to determine their relevance to obesity and heart disease. Studies that did not involve human populations, including animal and microbial studies, were also excluded. As a result, a final sample of 28,315 documents was included in the study. Further details on the process of document selection and retrieval can be found in Figure 1.
BIBLIOMETRIC INDICATORS
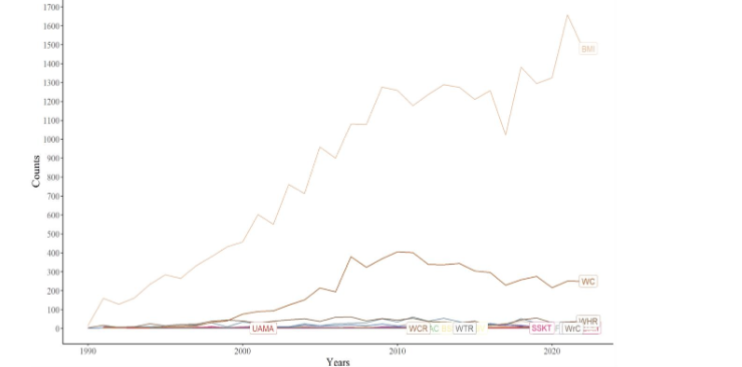
The study used a bibliometric approach, a quantitative method used to analyse patterns and trends in literature. Two (quantity, and intellectual) broad bibliometric analysis measures were documented in the study. First, the quantity index, comprised the identification of health-related documents via WOS contextually trends in obesity and heart disease studies, distribution of biomarkers, anthropometric indices and comorbidities of obesity and heart disease, and second index, intellectual, focused on the topics and themes from abstracts and distribution of the topics across various countries and regions of the world. To overcome potential alterations in obesity and heart disease search results, the study used data retrieved on the 3rd June 2023.
STATISTICAL ANALYSIS
Data management and analysis were conducted using R software. R programme is a software environment and programming language designed for statistical analysis, graphical representation, and data reporting. To conduct bibliometric analysis, the dplyr, bibliometrix, quanteda, wosr, tidyr, tidybib, and ggplot2 R packages for the analysis were utilised. The text underwent grammatical manipulation using dplyr. The WOS text was transformed from a bib file to R-readable text using bibliometrix, wosr, and tidybib. Quanteda and tidyr were employed for the topic modeling analysis. All plots were generated using ggplot2. The study described and modelled topics using the WOS documents to shed light on the research landscape surrounding obesity and heart disease from the extant literature. For the descriptive analysis (trends in obesity and heart disease research per location and the biomarkers, anthropometric indices and comorbidities inclusivity by year of publication and location) were estimated. The anthropometric indices, biomarkers, and comorbidities employed for monitoring the indices across different countries of origin and each research document are detailed in Table 1, presented in the appendix.
RESULTS
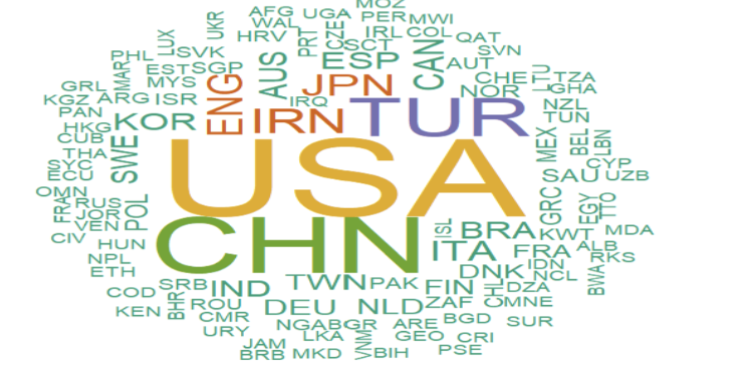
Figure 2 provides a comprehensive depiction of the evolving research landscape concerning obesity and heart disease spanning the extensive timeframe from 1970 to 2022. During the initial years, a limited number of studies addressed these health issues, with a notable concentration in North America and Europe. The pivotal shift occurred around 1990, marking a substantial upswing in research activity, particularly in these aforementioned regions. Despite the heightened global interest, the epicentre of publications remained entrenched in North America, Europe, and extended to Central Asia, East Asia, and the Pacific regions. Conversely, Sub-Saharan Africa and South Asia witnessed a gradual increase in research output, reaching a noteworthy inflection point in the years following 2015. This intricate timeline underscores the nuanced regional dynamics and evolving research emphasis on obesity and heart disease over the decades.
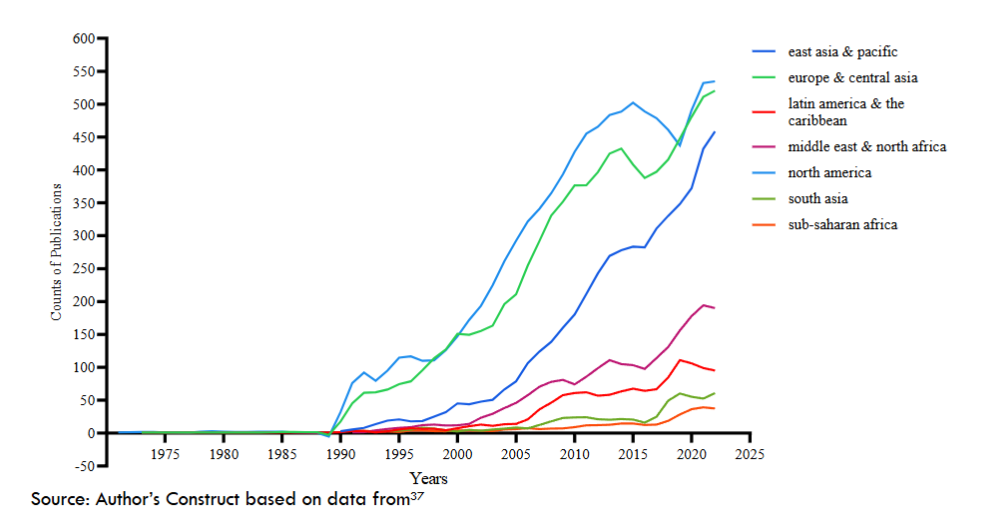
Table 1: Topics in Obesity and Heart Disease Research
| Topics | Content | Emerging themes |
|---|---|---|
| 1 | active, physical, related, intake, behaviour, lifestyle, report, fruits, find, food, evc, exercise, well, fatty, alcohol | impact of lifestyle on health outcomes |
| 2 | age, year, participate, adult, individual, score, mean, older, base, data, estimate, sex, follow, cohort, status | population characteristics and analysis |
| 3 | bmi, body, index, mass, kg, overweight, normal, whtr, measure, greater, mean, respective, higher, increase, total | anthropometric indices and measurements |
| 4 | weight, change, increase, effect, improve, decrease, treatment, week, day, intervention, reduce, loss, month, term, reduction | weight change and intervention |
| 5 | women, men, prevalence, among, population, higher, age, countries, educate, survey, geospatial, sampling, differ, cross, sex | gender- and country-specific prevalence rates |
| 6 | blood, pressure, male, subject, female, hypertension, systolic, diastolic, left ventricular function, significant, mean, arteries, parameter | biomarkers and population characteristics and health |
| 7 | patient, vs, clinic, failure, severe, hospital, chest, artery, outcome, without, include, breath, present, primarily, screening | cardiac health and the screening of patients |
| 8 | metabolic, insulin, syndrome, glucose, resist, increase, fast, subject, association, high, suggest, elevate, individual, marker, reserve | metabolic syndrome and insulin resistance as comorbidities |
| 9 | level, high, cholesterol, low, serum, lipid, hdl, total, lipoprotein, mg, plasma, densities, concentrate, triglyceride, resist | biomarkers |
| 10 | risk factor, circulatory, dse, chest, smoke, event, high, population, historical, major, tifi, prevent, known, include | cardiovascular risk factors and prevention |
| 11 | associate, measure, analysis, waist, independent, model, variable, circumference, relationship, regression, ratio, predict, correlate, assess, abdomen | methods and anthropometric indices for obesity assessment |
| 12 | diabetes, type, dse, pressure, high, chronic, develop, condition, mellitus, case, include, medication, disorder, common, morbid | chronic conditions and common comorbidities |
| 13 | associate, ci, mortal, adjust, ratio, grip, death, intervention, odds, ca, increase, cases, follow, model, multivariate | statistical modelling factors associated with mortality and interventions |
| 14 | group, significant, control, compare, differ, rate, higher, lower, two, test, non, similar, show, found, statistics | statistical modelling |
| 15 | fat, diet, visceral, increase, adipose tissue, expression, function, induced, effect, acidic, protein, high, mechanised, response | risk factors and adipose |
Source: Author’s Construct based on data from the study.
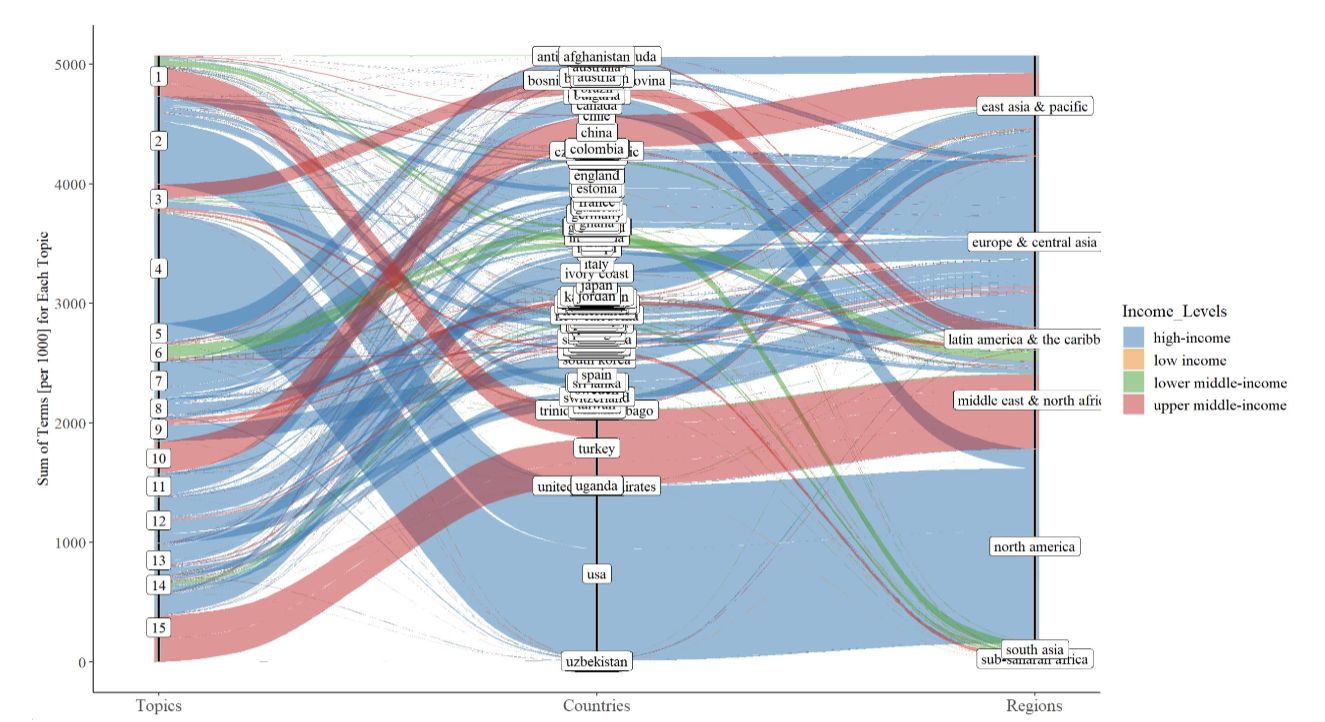
Table 2: Number of Anthropometric Indices, Biomarkers and Comorbidities Studied as Part of Obesity and Heart Disease Research
| Indicators Identified | No. Anthropometric Index Count | Biomarkers Count | Comorbidities Count | ||
|---|---|---|---|---|---|
| 1 ankle circumference (AC) | 1 | adiponectin | 1111 | atrial fibrillation | 952 |
| 2 arm fat area (AFA) | 10 | apolipoprotein a1 | 126 | depression and anxiety disorders | 2 |
| 3 android fat distribution (AFD) | 14 | apolipoprotein b | 604 | diabetes/ diabetes mellitus /mellitus | 20756 |
| 4 abdominal girth (AG) | 18 | brain natriuretic peptide (BNP) | 313 | metabolic syndrome | 8124 |
| 5 arm muscle circumference (AMC) | 12 | cholesterol | 7796 | sleep apnea | 834 |
| 6 body adiposity index (BAI) | 48 | c-reactive protein (CRP) | 1838 | stroke | 3636 |
| 7 body density (BD) | 4 | fasting plasma glucose | 1658 | ||
| 8 body fat percentage (BFP) | 443 | fibrinogen | 523 | ||
| 9 body mass index (BMI) | 24322 | galectin-3 | 44 | ||
| 10 basal metabolic rate (BMR) | 38 | growth differentiation factor 15 (GDF-15) | 17 | ||
| 11 body surface area (BSA) | 164 | glycated haemoglobin | 217 | ||
| 12 body shape index (BSI) | 31 | haemoglobin a1c (HBa1c) | 692 | ||
| 13 calf circumference (CC) | 17 | high-density lipoprotein (HDL) | 1273 | ||
| 14 chest circumference (CC) | 4 | high-sensitivity cardiac troponin t | 15 | ||
| 15 conicity index (CI) | 99 | insulin | 7238 | ||
| 16 hip circumference (HC) | 864 | interleukin-1 beta | 28 | ||
| 17 lean body mass (LBM) | 461 | interleukin-6 | 954 | ||
| 18 mid-upper arm circumference (MUAC) | 16 | low-density lipoprotein (LPL) | 2990 | ||
| 19 neck circumference (NC) | 136 | lipoprotein | 9239 | ||
| 20 sagittal abdominal diameter (SAD) | 59 | matrix metalloproteinases | 15 | ||
| 21 skeletal muscle mass (SMM) | 73 | myeloperoxidase | 31 | ||
| 22 subscapular skinfold thickness (SSKT) | 68 | nt-probnp | 326 | ||
| 23 total body fat mass (TBFM) | 45 | resistin | 237 | ||
| 24 thigh circumference (TC) | 30 | soluble st2 | 15 | ||
| 25 visceral adiposity index (VAI) | 82 | tnf-alpha | 373 | ||
| 26 waist circumference (WC) | 6748 | total cholesterol | 3071 | ||
| 27 waist-to-hip ratio (WHR) | 1232 | troponin | 115 | ||
| 28 waist-to-thigh ratio (WTR) | 24 | troponin i | 45 | ||
| 29 wrist circumference (WrC) | 7 | tumour necrosis factor-alpha | 155 |
Discussion
The paper provides an analysis of the literature on obesity and heart disease in the world. The analysis further enhances the understanding of the trends, topics, geospatial contributions in and to obesity and heart disease research. Using bibliometric approach and the PRISMA method and data retrieved from WOS, the study revealed several important insights.
The compelling insights derived from Figure 2 illuminate the dynamic trajectory of research endeavours surrounding obesity and heart disease from 1970 to 2022. The initial scarcity of studies, predominantly confined to North America and Europe, echoes the historical focus of these regions in health research. However, the pivotal juncture around 1990 signifies a paradigm shift, witnessing a substantial surge in research activities, especially within the mentioned regions. The current finding is unsurprising given the history of agencies and institutions of the US, Canada and European countries, in conducting and implementing health research, including other analogous academic health programmes.
Despite the escalating global interest in the subject, the sustained dominance of North America and Europe in scholarly contributions is evident. The dissemination of research influence expands beyond these regions to encompass Central Asia, East Asia, and the Pacific, indicating a broadening scope. In contrast, Sub-Saharan Africa and South Asia, while experiencing a gradual rise in research output, demonstrate a significant inflection point post-2015, reflecting a belated yet impactful engagement with the subject matter. This outcome serves as a clear call to action for developed countries to extend their support and promote research endeavours in the developing regions of the world. This is particularly crucial as there is an upsurge in the prevalence of obesity and heart disease, especially in Sub-Saharan Africa and Southeast Asia. In Sub-Saharan Africa alone, obesity is projected to cause 80,000,000 years of life loss within two decades, that is, 2040. Also, the end of this decade, countries in Sub-Saharan Africa and Southeast Asia will host about 75% and 80% all global hypertension and diabetes cases due to obesity. Consequently, the primary focus should be on encouraging developed nations to invest in and enhance research infrastructure, and initiate research networks with scientists in developed countries. Obesity rates are on the rise in LMICs, impacting various indices including the widespread use of BMI as the main tool for screening health. This facilitates the surge in understanding obesity and use of specific user-friendly indices for its assessment. The surge in obesity research is in parallel with several factors, including changing diets, economic transitions, socioeconomic disparities, and marketing influences. As a result, obesity research in LMICs aims to better understand these contributing factors and their impact on various indices. The shift in focus over the decades reflects not only the changing landscape of global health priorities but also highlights the imperative for a more inclusive and diversified approach in understanding and addressing these critical health issues worldwide.
The majority of studies reviewed focused on health factors and medical conditions and outcomes. These themes encompassed a wide range of topics related to population characteristics, health indices, comorbidities associated with obesity and heart diseases, as well as lifestyle and behavioural factors. The emphasis on health factors highlights the significance of understanding the various determinants of health, including the investigation of population characteristics such as age, sex, and demographics in general. The inclusivity of such determinants provide insights into the distribution and prevalence of obesity and heart diseases within different groups in conjunction with the identification of populations at higher risk for obesity and heart disease to enable targeted interventions. Similarly, the inclusion of demographics as part of obesity and heart disease research reveals a shift from considering obesity and heart disease as individual challenges to recognising them as afflictions of population groups. This shift underscores the urgency in developing preventive strategies that can reach a larger number of people. Moreover, health indices played a crucial role in these studies, allowing researchers to assess and measure factors like body weight, body mass index (BMI), blood pressure, and lipid profiles. These indices serve as valuable markers for evaluating the health status and identifying potential risks associated with obesity and heart diseases. It may also be speculated that the focus on biomarkers and anthropometric indices in research studies is due to the need to evaluate disease treatment efficacy. Assessing differing biomarkers and anthropometric indices for obesity and heart diseases can reveal the measures that are most effective for various populations’ health assessment and treatment. This, in turn, provides a deeper understanding of the pathophysiology of obesity and heart diseases, paving the way for new discoveries and innovations in treatment and prevention.
Comorbidities, which refer to the simultaneous presence of multiple health conditions, were also explored extensively. Incorporating obesity, disease markers, and comorbidities is crucial for understanding how obesity and heart diseases interact to exacerbate other conditions. These insights may reveal shared risk factors or underlying mechanisms driving their cause and effect relationship, as well as the overall health consequences for individuals and population groups affected by both obesity and heart disease. Plus, that knowledge triggers the development of effective disease management strategies such that health care providers can better manage patients with both conditions when they perceive their confluence and potential complications. Like the indicators above, lifestyle and behavioural factors emerged as important themes within literature. These encompassed aspects such as physical activity levels, dietary habits, smoking, and other behaviours that influence the development and progression of obesity and heart diseases. Investigating these factors helps in identifying modifiable risk factors and designing interventions to promote healthier lifestyles.
Conclusion
The study highlights the valuable insights provided by the identified research topics in the field of obesity and heart disease. It emphasises the importance of considering population characteristics, health assessment, comorbidities, and lifestyle factors when addressing these conditions. Taking a holistic approach is crucial for developing comprehensive strategies that effectively tackle the complexity of obesity and heart disease. The study suggests that leveraging the findings can aid policymakers, healthcare professionals, and researchers in prioritizing evidence-based interventions and collaborations to mitigate the burden of obesity and heart disease. Continued research, international cooperation, and interdisciplinary efforts are deemed essential to develop effective prevention and intervention strategies, especially in regions with limited research activity. Addressing obesity and heart disease requires a multifaceted approach that includes education, policy changes, improvement in healthcare systems, and community engagement. Working together, it is concluded that we strive towards a healthier future and reduce the impact of obesity and heart disease on individuals, communities, and societies as a whole.
Declarations
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not Applicable
CONFLICTS OF INTERESTS
The authors declare that there are no competing interests.
FUNDING
This study received no external funding. However, the authors sincerely thank Bielefeld University, Germany, for providing financial support through the Institutional Open Access Publication Fund for the article processing charge (APC).
AUTHOR’S CONTRIBUTIONS
SSS conceived the study. SSS and JEH drafted the manuscript. SSS, JEH, MSS, and TS read, and approved intellectual content of the final manuscript.
DATA AVAILABILITY
The data used for the study is available at: Web of Science
Appendix
Table 1: Anthropometric indices, biomarkers and comorbidities to be identified
| Index Name | Abbreviation |
|---|---|
| Arm muscle circumference | AMC |
| Arm fat area | AFA |
| Body density | BD |
| Bone density | BD* |
| Basal metabolic rate | BMR |
| Body surface area | BSS |
| Blood volume | BV |
| Bone mineral content | BMC |
| Bone mineral density | BMD |
| Chest circumference | CC |
| Chest-to-hip ratio | CHR |
| Calf circumference | CL |
| Elbow breadth | EB |
| Gluteofemoral fat mass | GFD |
| Hip circumference | HC |
| Hip-to-height ratio | HHR |
| Knee breadth | KB |
| Lean body mass | LBM |
| Skeletal muscle mass | SMM |
| Standing height | STR |
| Thigh circumference | TC |
| Thigh-to-calf ratio | TCR |
| Trunk length | TL |
| Waist circumference | WC |
| Waist-to-hip ratio | WCR |
| Waist-to-height ratio | WHR |
| Waist-to-hip-to-thigh ratio | WHTHR |
| Waist-to-hip-to-trunk ratio | WHTR |
| Waist-to-thigh ratio | WTR |
Biomarkers
| Index Name | Abbreviation |
|---|---|
| C-reactive protein | CRP |
| Natriuretic peptides | – |
| B-type natriuretic peptide | BNP |
| N-terminal pro-B-type natriuretic peptide | NT-proBNP |
| High-sensitivity cardiac troponin | – |
| Troponin | – |
| Insulin | – |
| Lipoprotein | – |
| Triglycerides | – |
| Cholesterol | – |
| Total cholesterol | – |
| LDL cholesterol | LDL |
| HDL cholesterol | HDL |
| Apolipoprotein B | ApoB |
| Apolipoprotein A1 | ApoA1 |
| Adiponectin | – |
| Resistin | – |
| Tumor necrosis factor-alpha | TNF-alpha |
| Interleukin-6 | IL-6 |
| Interleukin-1 beta | IL-1β |
Comorbidities
| Index Name | Abbreviation |
|---|---|
| Fasting plasma glucose/ Fasting blood glucose | FPG |
| Diabetes mellitus | – |
| Hypertension | – |
| Hyperlipidemia | – |
| Obesity | – |
| Coronary artery disease | – |
| Stroke | – |
| Chronic kidney disease | – |
| Chronic obstructive pulmonary disease | – |
| Heart failure | – |
| Atrial fibrillation | – |
| Valvular heart disease | – |
| Arrhythmias | – |
| Metabolic syndrome | – |
| Sleep apnea | – |
References
1. Powell-Wiley TM, Poirier CP, Burke VCLE, Després, JP, Gordon-Larsen P, Lavie CJ, Lear SA, Ndumele CE, Neeland IJ, Sanders P, St-Onge MP. Obesity and cardiovascular disease. Circulation. 2021; 143(21): e984–e1010. https://doi.org/10.1161/CIR.0000000000000973
2. Adeboye B, Bermano G, Rolland C. Obesity and its health impact in Africa: A systematic review. Cardiovascular Journal of Africa. 2012; 23(9), 512–521. https://doi.org/10.5830/CVJA-2012-040
3. Asosega KA, Adebanji AO, Abdul IW. Spatial analysis of the prevalence of obesity and overweight among women in Ghana. BMJ Open. 2021; 11(1), e041659. https://doi.org/10.1136/bmjopen-2020-041659
4. Atek M, Traissac P, El Ati J, Laid Y, Aounallah-Skhiri H, Eymard-Duvernay S, Mézimèche N, Bougatef S, Béji C, Boutekdjiret L, Martin-Prével Y, Lebcir H, Gartner A, Kolsteren P, Delpeuch F, Romdhane HB, Maire B. Obesity and association with area of residence, gender and socio-economic factors in Algerian and Tunisian adults. PLoS ONE. 2013; 8(10), e75640. https://doi.org/10.1371/journal.pone.0075640
5. Dhana K, Ikram MA, Hofman A, Franco OH, Kavousi M. Anthropometric measures in cardiovascular disease prediction: Comparison of laboratory-based versus non-laboratory-based model. Heart . 2015; 101(5), 377–383. https://doi.org/10.1136/heartjnl-2014-306704
6. Liu , Tse LA, Liu Z, Rangarajan S, Hu B, Yin L, Leong DP, Li W, Liu B, Chen C, Jin G, Zhang H, Chen H, Bo J, Li J, Li J, Yang J, Wang K, Zhang L, Yang S. Predictive values of anthropometric measurements for cardiometabolic risk factors and cardiovascular diseases among 44 048 Chinese. Journal of the American Heart Association. 2019; 8(16), e010870. https://doi.org/10.1161/JAHA.118.010870
7. Cercato C, Fonseca FA. Cardiovascular risk and obesity. Diabetology & Metabolic Syndrome. 2019; 11(1), 74. https://doi.org/10.1186/s13098-019-0468-0
8. Hruby A, Hu FB. The Epidemiology of obesity: A big picture. PharmacoEconomics. 2015; 33(7), 673–689. https://doi.org/10.1007/s40273-014-0243-x
9. Loos RJF, Yeo GSH. The genetics of obesity: From discovery to biology. Nature Reviews Genetics. 2022; 23(2), Article 2. https://doi.org/10.1038/s41576-021-00414-z
10. Piqueras P, Ballester A, Durá-Gil JV, Martinez-Hervas S, Redón J, Real JT. Anthropometric indicators as a tool for diagnosis of obesity and other health risk factors: A literature review. Frontiers in Psychology. 2021; 12, 631179. https://doi.org/10.3389/fpsyg.2021.631179
11. Mayeux R. Biomarkers: Potential uses and limitations. NeuroRx. 2004; 1(2), 182–188.
12. Al Kibria GM, Burrowes V, Choudhury A, Sharmeen A, Swasey K. Sex differences in prevalence and associated factors of prehypertension and hypertension among Bangladeshi adults. International Journal of Cardiology Hypertension. 2019; 1, 100006. https://doi.org/10.1016/j.ijchy.2019.100006
13. Simmons SS, Hagan JrJE, Schack T. The Influence of anthropometric indices and intermediary determinants of hypertension in Bangladesh. International Journal of Environmental Research and Public Health. 2021; 18(11), 5646. https://doi.org/10.3390/ijerph18115646
14. Tharkar S, Viswanathan V. Effect of obesity on cardiovascular risk factors in urban population in South India. Heart Asia, 2010; 2(1), 145–149. https://doi.org/10.1136/ha.2009.000950
15. Pritchard A. Statistical bibliography or bibliometrics. Journal of Documentation. 1969. https://www.semanticscholar.org/paper/Statistical-bibliography-or-bibliometrics-Pritchard/0be426317b9001813ece55e91c77281e9bd48205
16. Birkle C, Pendlebury DA, Schnell J, Adams J. Web of science as a data source for research on scientific and scholarly activity. Quantitative Science Studies. 2020; 1(1), 363–376. https://doi.org/10.1162/qss_a_00018
17. Hossain S, Batcha MS, Atoum I, Ahmad N, Al-Shehri A. Bibliometric analysis of the scientific research on sustainability in the impact of social media on higher education during the covid-19 pandemic. Sustainability. 2022; 14(24), Article 24. https://doi.org/10.3390/su142416388
18. Gao Y, Wang Y, Zhai X, He Y, Chen R, Zhou J, Li M, Wang Q. (2017). Publication trends of research on diabetes mellitus and T cells (1997–2016): A 20-year bibliometric study. PLOS ONE. 2017; 12(9), e0184869. https://doi.org/10.1371/journal.pone.0184869
19. Sweileh WM, Al-Jabi SW, Sawalha AF, Zyoud SH. Bibliometric analysis of nutrition and dietetics research activity in Arab countries using ISI Web of science database. SpringerPlus 2014; 3, 718. https://doi.org/10.1186/2193-1801-3-718
20. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ. 2015; 349, g7647. https://doi.org/10.1136/bmj.g7647
21. Garfield E. Citation analysis as a tool in journal evaluation. Science. 1972; 178(4060), 471–479. https://doi.org/10.1126/science.178.4060.471
22. Aria M, Cuccurullo C. Bibliometrix: Comprehensive science mapping analysis (4.1.2) [Computer software]. 2023.
https://CRAN.R-project.org/package=bibliometrix
23. Barnier J. R interface with web of science web services API [R]. 2021. https://github.com/juba/rwos (Original work published 2017)
24. Benoit K. Watanabe K, Wang H, Nulty P, Obeng A, Müller S, Matsuo A. quanteda: An R package for the quantitative analysis of textual data. Journal of Open Source Software. 2018; 3(30), 774. https://doi.org/10.21105/joss.00774
25. Donny. Tidy bib, the art of typesetting [Python]. 2022. https://github.com/MrDongdongLin/tidybib (Original work published 2019)
26. Wickham H. ggplot2: Elegant graphics for data analysis (2nd ed.). 2009. Springer Publishing Company, Incorporated.
27. Wickham H, François R, Henry L, Müller K, RStudio. dplyr: A grammar of data manipulation (1.0.4) [Computer software]. 2021. https://CRAN.R-project.org/package=dplyr
28. Noble PJM, Appleton C, Radford AD, Nenadic G. Using topic modelling for unsupervised annotation of electronic health records to identify an outbreak of disease in UK dogs. PLoS ONE. 2021; 16(12), e0260402. https://doi.org/10.1371/journal.pone.0260402
29. Ray SK, Ahmad A, Kumar CA. Review and implementation of topic modeling in Hindi. Applied Artificial Intelligence. 2019; 33(11), 979–1007. https://doi.org/10.1080/08839514.2019.1661576
30. Salloum SA, Al-Emran M, Monem AA, Shaalan K. (2018). Using Text Mining Techniques for Extracting Information from Research Articles. In K. Shaalan, A. E. Hassanien, & F. Tolba (Eds.), intelligent natural language processing: Trends and applications. Springer International Publishing. 2018; 740, 373–397. https://doi.org/10.1007/978-3-319-67056-0_18
31. Sharma N, Bairwa M, Gowthamghosh B, Gupta SD, Mangal DK. A bibliometric analysis of the published road traffic injuries research in India, post-1990. Health Research Policy and Systems. 2018; 16(1), 18. https://doi.org/10.1186/s12961-018-0298-9
32. Wang SH, Ding Y, Zhao W, Huang YH, Perkins R, Zou W, Chen JJ. Text mining for identifying topics in the literatures about adolescent substance use and depression. BMC Public Health. 2016; 16(1), 279. https://doi.org/10.1186/s12889-016-2932-1
33. Valenti AP, Bock AW. Using topic modeling to infer the emotional state of people living with Parkinson’s disease. Assistive Technology. 2019; 0(0), 1–10. https://doi.org/10.1080/10400435.2019.1623342
34. Blei DM, Ng AY, Jordan MI. Latent dirichlet allocation. The Journal of Machine Learning Research. 2003; 3(null), 993–1022.
35. Liu L, Tang L, Dong W, Yao S, Zhou W. An overview of topic modeling and its current applications in bioinformatics. SpringerPlus. 2016; 5(1), 1608. https://doi.org/10.1186/s40064-016-3252-8
36. Rijcken E, Kaymak U, Scheepers F, Mosteiro P, Zervanou K, Spruit M. Topic modeling for interpretable text classification from EHRs. Frontiers in Big Data. 2022; 5. https://www.frontiersin.org/articles/10.3389/fdata.2022.846930
37. Web of Science. Document search—Web of science core collection. 2022. https://www.webofscience.com/wos/woscc/basic-search
38. Bai A, Wu C, Yang K. Evolution and features of China’s central government funding system for basic research. Frontiers in Research Metrics and Analytics. 2021; 6. https://www.frontiersin.org/articles/10.3389/frma.2021.751497
39. Charani E, Abimbola S, Pai M, Adeyi O, Mendelson M, Laxminarayan R, Rasheed MA. Funders: The missing link in equitable global health research? PLOS Global Public Health. 2022; 2(6), e0000583. https://doi.org/10.1371/journal.pgph.0000583
40. Franzen SRP, Chandler C, Lang T. Health research capacity development in low and middle income countries: Reality or rhetoric? A systematic meta-narrative review of the qualitative literature. BMJ Open. 2017; 7(1), e012332. https://doi.org/10.1136/bmjopen-2016-012332
41. Head MG, Brown RJ, Newell ML, Scott JAG, Batchelor J, Atun R. The allocation of US$105 billion in global funding from G20 countries for infectious disease research between 2000 and 2017: A content analysis of investments. The Lancet Global Health. 2020; 8(10), e1295–e1304. https://doi.org/10.1016/S2214-109X(20)30357-0
42. Knai C, Gilmore A, Lock K, McKee M. Public health research funding: Independence is important. The Lancet. 2010; 376(9735), 75–77. https://doi.org/10.1016/S0140-6736(09)62063-8
43. Yegros-Yegros A, van de Klippe W, Abad-Garcia MF, Rafols I. Exploring why global health needs are unmet by research efforts: The potential influences of geography, industry and publication incentives. Health Research Policy and Systems. 2020; 18, 47. https://doi.org/10.1186/s12961-020-00560-6
44. Sitthi-amorn C, Somrongthong R. Strengthening health research capacity in developing countries: A critical element for achieving health equity. BMJ : British Medical Journal. 2000; 321(7264), 813–817.
45. Syed SB, Dadwal V, Rutter P, Storr J, Hightower JD, Gooden R, Carlet J, Nejad SB, Kelley ET, Donaldson L, Pittet D. Developed-developing country partnerships: Benefits to developed countries? Globalization and Health. 2012; 8(1), 17. https://doi.org/10.1186/1744-8603-8-17
46. Shrum W, Campion P. Are scientists in developing countries isolated? Science, Technology and Society. 2000; 5(1), 1–34. https://doi.org/10.1177/097172180000500101
47. Van der Veken K, Belaid L, Delvaux T, De Brouwere V. Research capacity building through North–South–South networking: Towards true partnership? An exploratory study of a network for scientific support in the field of sexual and reproductive health. Health Research Policy and Systems. 2017; 15(1), 39. https://doi.org/10.1186/s12961-017-0202-z
48. Simmons SS. Strikes and Gutters: Biomarkers and anthropometric measures for predicting diagnosed diabetes mellitus in adults in low- and middle-income countries. Heliyon. 2023; 9(9), e19494. https://doi.org/10.1016/j.heliyon.2023.e19494
49. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, Adams RJ, Aekplakorn W, Afsana K, Aguilar-Salinas CA, Agyemang, C, Ahmadvand A, Ahrens W, Ajlouni K, Akhtaeva N, Al-Hazzaa HM, Al-Othman AR, Al-Raddadi R, Buhairan FA, … Ezzati M. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128•9 million children, adolescents, and adults. The Lancet. 2017; 390(10113), 2627–2642. https://doi.org/10.1016/S0140-6736(17)32129-3
50. Ford ND, Patel SA, Narayan KMV. Obesity in low- and middle-income countries: burden, drivers, and emerging challenges. Annual Review of Public Health. 2017; 38(1), 145–164. https://doi.org/10.1146/annurev-publhealth-031816-044604
51. Berwick DM. The Moral Determinants of Health. JAMA. 2020; 324(3), 225–226. https://doi.org/10.1001/jama.2020.11129
52. Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014; 129, 2(2):19-31. doi: 10.1177/00333549141291S206.
53. Health IIC, Durch JS, Bailey L.A, Stoto MA. Understanding health and Its determinants. In Improving health in the community: A role for performance monitoring. National Academies Press (US). 1997. https://www.ncbi.nlm.nih.gov/books/NBK233009/
54. Hussain A, Ali I, Kaleem WA, Yasmeen F. Correlation between Body Mass Index and Lipid Profile in patients with Type 2 Diabetes attending a tertiary care hospital in Peshawar. Pakistan Journal of Medical Sciences. 2019; 35(3), 591–597.` https://doi.org/10.12669/pjms.35.3.7
55. Capodaglio P, Lafortuna C, Petroni ML, Salvadori A, Gondoni L, Castelnuovo G, Brunani A. Rationale for hospital-based rehabilitation in obesity with comorbidities. European Journal of Physical and Rehabilitation Medicine. 2013; 49(3), 399–417.
56. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: Implications for understanding health and health services. Annals of Family Medicine. 2009; 7(4), 357–363. https://doi.org/10.1370/afm.983
57. Amankwah-Poku, M. A cross-sectional study of knowledge and awareness of type 2 diabetes mellitus in a student population in Ghana: Do demographics and lifestyle make a difference. Health Psychology and Behavioral Medicine. 2019; 7(1), 234–252. https://doi.org/10.1080/21642850.2019.1637261
58. Anto EO, Owiredu WKBA, Adua, E, Obirikorang C, Fondjo LA, Annani-Akollor ME, Acheampong E, Asamoah EA, Roberts P, Wang W, Donkor S. Prevalence and lifestyle-related risk factors of obesity and unrecognized hypertension among bus drivers in Ghana. Heliyon. 2020; 6(1), e03147. https://doi.org/10.1016/j.heliyon.2019.e03147
59. Bittner V, Simon JA, Fong J, Blumenthal RS, Newby K, Stefanick ML. Correlates of high HDL cholesterol among women with coronary heart disease. American Heart Journal. 2000; 139(2), 288–296. https://doi.org/10.1067/mhj.2000.101224
60. Cockerham WC. Health lifestyle theory and the convergence of agency and structure. Journal of Health and Social Behavior. 2005; 46(1), 51–67. https://doi.org/10.1177/002214650504600105
61. Fett CA, Rezende Fett WC, Marchini JS, Pessa Ribeiro RP. Lifestyle and risk factors associated to body fat increase in women. Ciencia & Saude Coletiva. 2010; 15(1), 131–140. https://doi.org/10.1590/S1413-81232010000100019
62. Hu FB. Globalization of Diabetes: The role of diet, lifestyle, and genes. Diabetes Care. 2011; 34(6), 1249–1257. https://doi.org/10.2337/dc11-0442
63. Kim EJ, Cho SW, Kang JY, Choi TI, Park YK. Effects of a 12-week lifestyle intervention on health outcome and serum adipokines in middle-aged korean men with borderline high blood pressure. Journal of the American College of Nutrition. 2012; 31(5), 352–360. https://doi.org/10.1080/07315724.2012.10720440
64. Haustein S, Larivière V. The Use of Bibliometrics for assessing research: Possibilities, limitations and adverse effects. In IM Welpe, J Wollersheim, S Ringelhan, M Osterloh (Eds.), Incentives and performance: Governance of research organizations. Springer International Publishing. 2015; 121–139. https://doi.org/10.1007/978-3-319-09785-5_8
65. Kivimäki, M., Strandberg, T., Pentti, J., Nyberg, S. T., Frank, P., Jokela, M., Ervasti, J., Suominen, S. B., Vahtera, J., Sipilä, P. N., Lindbohm, J. V., & Ferrie, J. E. (2022). Body-mass index and risk of obesity-related complex multimorbidity: An observational multicohort study. The Lancet Diabetes & Endocrinology, 10(4), 253 -263. https://doi.org/10.1016/S2213-8587(22)00033-X