





Patient Satisfaction with Telehealth Post-Lung Resection
Patient Satisfaction with Telephone Follow-up after Lung Resection: Are we making the right ‘call’?
1. Introduction:
In response to the coronavirus 2019 (COVID-19) pandemic, most institutions saw increased utilization of telemedicine¹˒². Despite comparable satisfaction rates, patient attitudes toward telemedicine as an alternative during COVID-19 appear mixed as some studies indicate the majority of patients would still prefer in-person healthcare³˒⁴. Moreover, in the first half of 2020, only 6.6% of articles published on telehealth use during COVID-19 were in surgical fields⁵. Most surgical studies have focused on telemedicine utilization for pre-operative consultations and during the immediate postoperative period. Few studies have looked at the use of telemedicine in the postoperative surveillance of cancer patients after discharge⁶˒⁸. To our knowledge, there exists only a single study evaluating the use of telehealth among patients undergoing lung resection. Cerfolio et al. included 56 patients who underwent remote video-based communication pre-operatively and post-operatively and reported comparable morbidity to patients receiving in-person visits, as well as high patient satisfaction rates⁶. A limitation of their research was the limited number of patients who received telemedicine follow-ups in the post-operative setting (45%) and that patient’s did not have an initial in-person visit to compare their telehealth experience with. Understanding how patient and clinician perceptions toward telehealth change in the postoperative period is important to determine the appropriateness of this adjunct to clinical care during and beyond the COVID-19 pandemic.
The objective of this study was to examine patient satisfaction with telephone follow-up after lung resection for lung cancer during the pandemic. Through conducting this research, we aimed to better understand our patients’ levels of concern about COVID-19, its perceived impact on their medical care, and their views on the use of telemedicine technology post-pandemic.
2. Methods:
2.1 STUDY DESIGN:
A single-site, retrospective study was carried out by three academic thoracic surgeons performing telephone-based follow-up appointments. All lung cancer patients undergoing a post-operative telephone follow-up between April to November 2020 who had also previously completed at least one in-person pre-operative visit or follow-up were invited to participate. An anonymous online survey was conducted using REDCap software hosted at the University of Alberta¹⁰. Participants were sent up to four automated reminder emails to complete the survey.
Our study’s primary outcome was patient satisfaction with telephone follow-ups, compared with in-person visits before COVID-19. Secondary outcomes included surveying patients’ levels of concern about COVID-19, its perceived impact on their medical care, and their views on the utility of telemedicine post-pandemic.
2.2 PATIENT SATISFACTION SURVEY:
We adapted our survey questions from the previously validated Telehealth Usability Questionnaire¹¹ and several other forms¹²˒¹⁵ to align with our study context. Questions captured patients’ basic demographics, health status, previous telemedicine experience, COVID-19 concerns, and their perception of the efficiency, usefulness, quality of interaction, and satisfaction with telephone and in-person appointments. Questions were posed with a 5-point Likert scale from strongly disagree (1) to strongly agree (5).
2.3 STATISTICAL ANALYSIS:
The McNemar and Stuart-Maxwell tests for paired data with two, or more than two, categorical dependent variables, respectively, were used to compare satisfaction metrics of in-person and telephone appointments. For non-paired categorical data, Pearson’s Chi-square test of independence was used to evaluate if patient sex, education level, or health status affected their preference for in-person versus telephone visits. Statistical analyses were performed using R package, version 4.0.5 (The R Foundation) and statistical significance was defined a priori as a p-value less than 0.05.
2.4 ETHICS:
Verbal consent was obtained from all patients before the survey was sent. All responses were anonymous, and participants could skip questions that they did not wish to answer. The study protocol was approved by the University of Alberta Health Research Ethics Board.
3. Results
A total of 54 participants were sent the survey, with 47 completing it for a response rate of 87%. The majority of respondents were female (63.8%), and the mean age was 66.1 years (Table 1). Regarding COVID-19, 85% (39/46) of respondents were “somewhat” or “very” concerned about the pandemic in general and 76% (34/45) reported similar concerns about in-person healthcare appointments (Table 2). Moreover, 69% (31/45) indicated concern about delay or cancellation of their medical follow-up visits and 93.6% (44/47) stated that they were able to get the necessary follow-up imaging and lab work completed prior to their telephone appointment.
Table 1. Basic demographic information of survey respondents.
| Respondent Characteristic | N (%) |
|---|---|
| Age, mean, years (SD) (N = 43) | 66.1 +/- 9.06 |
| Sex (N = 47) | |
| Female | 30 (63.8%) |
| Male | 17 (36.2%) |
| Education Level (N = 47) | |
| Some high school or less | 8 (17.0%) |
| High school diploma | 11 (23.4%) |
| Some college/university | 10 (21.3%) |
| Certificate/diploma/applied degree | 11 (23.4%) |
| Bachelor’s degree or higher | 7 (14.9%) |
| Overall Health (N = 47) | |
| Excellent | 5 (10.6%) |
| Very good | 20 (42.6%) |
| Good | 17 (36.2%) |
| Fair | 5 (10.6%) |
| Poor | 0 (0.0%) |
| Previous Telephone Appointments (N = 47) | |
| None | 29 (61.7%) |
| 1–2 | 16 (34.0%) |
| 3–4 | 2 (4.3%) |
| 5 or more | 0 (0.0%) |
| Purpose of Telephone Appointment (N = 46) | |
| Workup of new lung nodule | 0 (0.0%) |
| First follow-up after surgery | 2 (4.3%) |
| Ongoing follow-up within 1 year of surgery | 10 (21.7%) |
| Ongoing follow-up over 1 year since surgery | 34 (73.9%) |
Table 2. Perceived concerns about COVID-19 and impact on participants’ post-operative medical care.
| Concern during COVID-19 about | N (%) |
|---|---|
| Pandemic in general (N = 46) | |
| Not concerned | 7 (15.2%) |
| Somewhat concerned | 21 (45.7%) |
| Very concerned | 18 (39.1%) |
| Going to hospital for appointments (N = 45) | |
| Not concerned | 11 (24.4%) |
| Somewhat concerned | 20 (44.4%) |
| Very concerned | 14 (31.1%) |
| Going to hospital for imaging/tests (N = 45) | |
| Not concerned | 12 (26.7%) |
| Somewhat concerned | 23 (51.1%) |
| Very concerned | 10 (22.2%) |
| Delay or cancellation of follow-ups (N = 45) | |
| Not concerned | 14 (31.1%) |
| Somewhat concerned | 22 (48.9%) |
| Very concerned | 9 (20.0%) |
| Inability to get imaging/tests before follow-ups (N = 44) | |
| Not concerned | 17 (38.6%) |
| Somewhat concerned | 17 (38.6%) |
| Very concerned | 10 (22.7%) |
There was no significant difference in participant comfort level and openness to telephone follow-ups before and after the actual encounter (p = 0.08) (Figure 1). There was also no significant difference reported between in-person and telephone appointments on all paired satisfaction questions directly comparing the two (Table 3). Nearly all participants (43/46 = 93.5%) agreed or strongly agreed that they could hear the surgeon and the surgeon could hear them clearly over telephone and 84.4% (38/45) similarly felt that they could be assessed appropriately despite no in-person examination. Overall, 85.1% (40/47) reported “No difference” in communication ability between appointment types and the majority rated telephone “much more” (27/46 = 58.7%) or “somewhat more” (9/46 = 19.6%) convenient than in-person assessment. Participants were divided on their overall preference for appointment type post-pandemic as 42.2% (19/45) preferred continuing with telephone, 44.4% (20/45) preferred switching back to in-person, and 13.3% (6/45) preferred all in-person visits regardless of COVID-19. This was statistically independent of participant sex (p = 0.73), education level (p = 0.66), health status (p = 0.86), and age (p = 0.28) (Table 4).
Figure 1. Participants’ perceived comfort level with telephone follow-ups before and after their actual telephone appointment
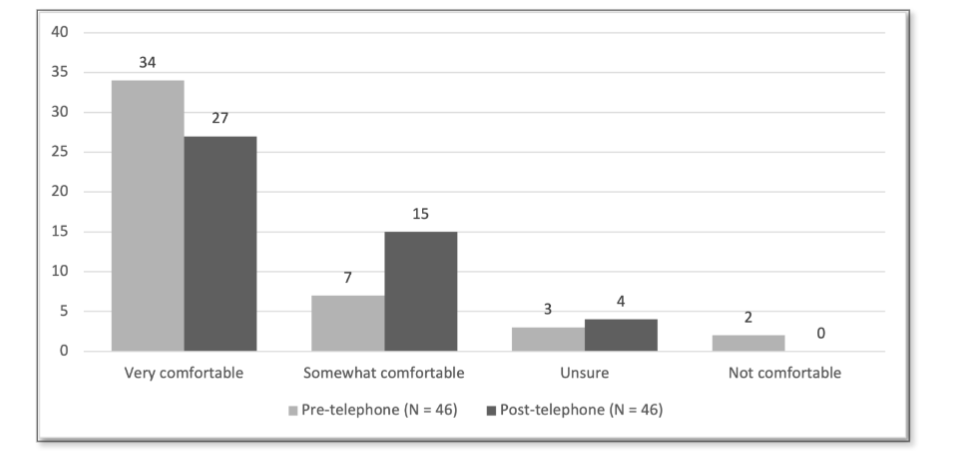
Table 3. Participant responses to paired questions directly comparing in-person versus telephone appointment experiences.
| Question | Clinic N (%) | Telephone N (%) | p-Value |
|---|---|---|---|
| My clinic/telephone appointment was (N = 45) | 0.45 | ||
| On-time | 39 (86.7%) | 42 (93.3%) | |
| Delayed (> 10 min.) | 6 (13.3%) | 3 (6.7%) | |
| I was comfortable sharing sensitive/personal information during my clinic/telephone appointment (N = 41) | 0.74 | ||
| Strongly agree | 25 (61.0%) | 23 (56.1%) | |
| Agree | 12 (29.3%) | 14 (34.1%) | |
| Neutral | 2 (4.9%) | 2 (4.9%) | |
| Disagree | 0 (0.0%) | 0 (0.0%) | |
| Strongly disagree | 2 (4.9%) | 2 (4.9%) | |
| I was able to effectively communicate my concerns during my clinic/telephone appointment (N = 40) | 0.59 | ||
| Strongly agree | 24 (60.0%) | 21 (52.5%) | |
| Agree | 13 (32.5%) | 15 (37.5%) | |
| Neutral | 1 (2.5%) | 2 (5.0%) | |
| Disagree | 0 (0.0%) | 0 (0.0%) | |
| Strongly disagree | 2 (5.0%) | 2 (5.0%) | |
| The surgeon could get a good understanding of my concerns during my clinic/telephone appointment (N = 41) | 0.43 | ||
| Strongly agree | 23 (56.1%) | 20 (48.8%) | |
| Agree | 15 (36.6%) | 16 (39.0%) | |
| Neutral | 1 (2.4%) | 3 (7.3%) | |
| Disagree | 0 (0.0%) | 0 (0.0%) | |
| Strongly disagree | 2 (4.9%) | 2 (4.9%) |
Table 4. Patients’ preferred type of follow-up encounter.
| Factor | All telephoneᵃ N (%) | Telephone & in-personᵇ N (%) | None & in-personᶜ N (%) | All & in-personᵈ N (%) | p-Value |
|---|---|---|---|---|---|
| All respondents | 19 (42.2%) | 20 (44.4%) | 0 (0.0%) | 6 (13.3%) | – |
| Sex | 0.73 | ||||
| Female | 11 (37.9%) | 14 (48.3%) | 0 (0.0%) | 4 (13.8%) | |
| Male | 8 (50.0%) | 6 (37.5%) | 0 (0.0%) | 2 (12.5%) | |
| Education | 0.66 | ||||
| Some high school or less | 5 (62.5%) | 3 (37.5%) | 0 (0.0%) | 0 (0.0%) | |
| High school diploma | 4 (36.4%) | 5 (45.5%) | 0 (0.0%) | 2 (18.2%) | |
| More than high school | 10 (38.5%) | 12 (46.2%) | 0 (0.0%) | 4 (15.4%) | |
| Health | 0.86 | ||||
| Excellent | 2 (40.0%) | 2 (40.0%) | 0 (0.0%) | 1 (20.0%) | |
| Very good | 7 (35.0%) | 10 (50.0%) | 0 (0.0%) | 3 (15.0%) | |
| Good | 7 (43.8%) | 7 (43.8%) | 0 (0.0%) | 2 (12.5%) | |
| Fair | 3 (75.0%) | 1 (25.0%) | 0 (0.0%) | 0 (0.0%) | |
| Poor | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
ᵃ All telephone follow-ups regardless of COVID-19
ᵇ Telephone follow-ups during COVID-19 and return to clinic post-pandemic
ᶜ No follow-ups during COVID-19 and return to clinic post-pandemic
ᵈ All clinic follow-ups regardless of COVID-19
4. Discussion
Our study evaluated patient satisfaction and suitability of telemedicine for longer-term postoperative cancer surveillance during the COVID-19 pandemic. Most participants in our study had no prior experience with telephone appointments and nearly three-quarters were being followed over 1-year since their surgery. As such, this study gauges the acceptability of telemedicine in a group of older, largely telemedicine-naïve patients, which reflects many of the lung cancer patients we see.
A majority of participants believed that they could still be assessed appropriately despite no physical exam, which is consistent with the literature¹⁶. Of note, they also found no difference in satisfaction between telephone and video-based forms of telemedicine. Importantly, and consistent with existing literature, our study showed that most patients found telephone to be “much more” or “somewhat more” convenient than clinic with no one reporting inferior convenience⁴˒¹⁷˒¹⁸. Despite this, studies have also demonstrated that a majority of patients would still prefer physical visits barring any restrictions, such as COVID-19, even though they were deemed to provide similar medical value³˒⁴˒⁶. Participants in our study did not become more comfortable with the idea of telephone encounters following their virtual appointment.
However, given the remarkable catalyst that COVID-19 has been for virtual technologies, we suspect increasing familiarity with telemedicine will lead to wider acceptance of this form of medical care. Furthermore, telemedicine may be better suited for longer-term follow-up as patients gain familiarity with their surgeon and the perceived complexity and acuity of follow-up visits decline over time.
A systematic review of the safety of telehealth usage in post-operative care supports our findings that virtual follow-up appointments are worth implementing in a post-pandemic world. The review emphasized the relative safety and efficiency of integrating virtual post-operative follow up appointments¹⁹. Virtual follow-up appointments were found to be just as safe as those done in person, with no difference in adverse event rates among patients receiving follow-up virtually. These findings combined with those of our study provide a strong foundation of support for telemedicine. A limitation discovered in the review was that many studies on telehealth had small sample sizes, which is similar to our own study. Another noted limitation of this review was the lack of controls for optimal comparison, which our study addresses with its within groups design, as each participant is able to act as a control for their own later responses on their virtual care. Lastly, the healthcare practitioners providing the virtual follow up appointments were nurses, while our study utilized surgeons.
Our study is limited by the small sample size and survey response bias, but these are balanced by the excellent response rate. Internet access was a prerequisite to participation, and we realize that access to a digital device with reliable internet and having sufficient knowledge to use it may bias the results of our study. Finally, a retrospective comparison of in-person versus telephone appointments may suffer from the recency effect, which could impact participant responses.
Despite these limitations, our study has a number of strengths, such as the within groups comparison of both telephone and in person experiences in medical care. A comparison of this nature highlights what patients think of both treatment options more directly as they have experienced both treatment effects. Furthermore, all patients received an in-person appointment first, allowing them to provide feedback on the virtual assessment after experiencing standard of care. The increased convenience and benefits of telemedicine for both patients and providers in the post-operative and surveillance period, as outlined in this study, supports the long-term feasibility of this modality of care. Further qualitative research is needed to better understand how in-person appointments seem to provide an increased sense of reassurance and if these components can be improved in the virtual setting. A hybrid model with both in-person and virtual appointments available based on patient preference may optimize patient satisfaction.
6. Conclusion:
Patient satisfaction with telephone follow-up after lung resection appears non-inferior to in-person appointments. The convenience of telemedicine for both patients and physicians may warrant sustained utilization of this modality of care post-pandemic.
Conflict of Interest:
None
Funding Statement:
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements:
None.
Author Contribution Statement:
Richard X. He: Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Writing – Original Draft.
Maxime Bédard: Data Curation, Formal Analysis, Investigation, Methodology, Writing – Original Draft.
Uzair Jogiat: Formal Analysis, Methodology, Writing – Review and Editing.
Simon R Turner: Conceptualization, Data Curation, Methodology, Writing – Review and Editing.
Eric L.R. Bédard: Conceptualization, Data Curation, Methodology, Writing – Review and Editing.
Azim Valji: Conceptualization, Data Curation, Methodology, Writing – Review and Editing.
Disclosures:
Simon Turner has a financial relationship with Astra-Zeneca and Ethicon.
Eric LR Bédard has a financial relationship with Astra-Zeneca and Hoffman La Roche.
Richard He, Maxime Bedard, Uzair Jogiat, and Azim Valji have no conflicts of interest to disclose.
References
1. Gilbert AW, Billany JCT, Adam R, et al. Rapid implementation of virtual clinics due to COVID-19: report and early evaluation of a quality improvement initiative. BMJ Open Qual 2020; 9. DOI: 10.1136/bmjoq-2020-000985.
2. Wosik J, Fudim M, Cameron B, et al. Telehealth transformation: COVID-19 and the rise of virtual care. J Am Med Inform Assoc 2020; 27: 957-962. DOI: 10.1093/jamia/ocaa067.
3. Chesnel C, Hentzen C, Le Breton F, et al. Efficiency and satisfaction with telephone consultation of follow-up patients in neuro-urology: Experience of the COVID-19 pandemic. Neurourol Urodyn 2021; 40: 929-937. 20210306. DOI: 10.1002/nau.24651.
4. Zhu C, Williamson J, Lin A, et al. Implications for Telemedicine for Surgery Patients After COVID-19: Survey of Patient and Provider Experiences. Am Surg 2020; 86: 907-915. 20200817. DOI: 10.1177/0003134820945196.
5. Doraiswamy S, Abraham A, Mamtani R, et al. Use of Telehealth During the COVID-19 Pandemic: Scoping Review. J Med Internet Res 2020; 22: e24087. 20201201. DOI: 10.2196/24087.
6. Cerfolio RJ, Ferrari-Light D and Shah S. Telemedicine in thoracic surgery. Journal of Visualized Surgery 2019; 5.
7. Humer MF and Campling BG. The Role of Telemedicine in Providing Thoracic Oncology Care to Remote Areas of British Columbia. Curr Oncol Rep 2017; 19: 52. DOI: 10.1007/s11912-017-0612-7.
8. Cleeland CS, Wang XS, Shi Q, et al. Automated symptom alerts reduce postoperative symptom severity after cancer surgery: a randomized controlled clinical trial. J Clin Oncol 2011; 29: 994-1000. 20110131. DOI: 10.1200/JCO.2010.29.8315.
9. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42: 377-381. 20080930. DOI: 10.1016/j.jbi.2008.08.010.
10. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 2019; 95: 103208. 20190509. DOI: 10.1016/j.jbi.2019.103208.
11. Parmanto B, Lewis AN, Jr., Graham KM, et al. Development of the Telehealth Usability Questionnaire (TUQ). Int J Telerehabil 2016; 8: 3-10. 20160701. DOI: 10.5195/ijt.2016.6196.
12. Viers BR, Lightner DJ, Rivera ME, et al. Efficiency, satisfaction, and costs for remote video visits following radical prostatectomy: a randomized controlled trial. Eur Urol 2015; 68: 729-735. 20150418. DOI: 10.1016/j.eururo.2015.04.002.
13. Dick PT, Filler R and Pavan A. Participant satisfaction and comfort with multidisciplinary pediatric telemedicine consultations. J Pediatr Surg 1999; 34: 137-141; discussion 141-132. DOI: 10.1016/s0022-3468(99)90244-0.
14. Demiris G, Speedie S and Finkelstein S. A questionnaire for the assessment of patients’ impressions of the risks and benefits of home telecare. J Telemed Telecare 2000; 6: 278-284. DOI: 10.1258/1357633001935914.
15. Newbould J, Abel G, Ball S, et al. Evaluation of telephone first approach to demand management in English general practice: observational study. BMJ 2017; 358: j4197. 20170927. DOI: 10.1136 /bmj.j4197.
16. Drerup B, Espenschied J, Wiedemer J, et al. Reduced No-Show Rates and Sustained Patient Satisfaction of Telehealth During the COVID-19 Pandemic. Telemed J E Health 2021; 27: 1409-1415. 20210304. DOI: 10.1089/tmj.2021.0002.
17. Gunter RL, Chouinard S, Fernandes-Taylor S, et al. Current Use of Telemedicine for Post-Discharge Surgical Care: A Systematic Review. J Am Coll Surg 2016; 222: 915-927. 20160213. DOI: 10.1016/j. jamcollsurg.2016.01.062.
18. Soegaard Ballester JM, Scott MF, Owei L, et al. Patient preference for time-saving telehealth postoperative visits after routine surgery in an urban setting. Surgery 2018; 163: 672-679. 201802 03. DOI: 10.1016/j.surg.2017.08.015.
19. Xiao K, Yeung JC and Bolger JC. The safety and acceptability of using telehealth for follow-up of patients following cancer surgery: A systematic review. Eur J Surg Oncol 2023; 49: 9-15. 20220909. DOI: 10.1016/j.ejso.2022.08.037.