
A comparison of volume and anthropometric breast measurements using the Crisalix and VECTRA XT 3-dimensional surface imaging systems in women who have undergone breast-conserving surgery
Main Article Content
Abstract
Introduction
Three-dimensional surface imaging (3D-SI) of the breasts enables the measurement of anthropometric distances and breast volume. These measurements may be used in surgical planning and to facilitate clear communication with patients. The aim of this study was to compare measurements using a portable 3D-SI system, Crisalix, with a more established non-mobile camera, the VECTRA XT.
Methods
Participants were imaged three times using the Crisalix and the VECTRA XT system. Breast volume, sternal notch to nipple distance, nipple to nipple distance and breast width were measured. Intra-observer agreement was measured using the co-efficient of variation (CV). Agreement between the two methods was represented with Bland Altman agreement plots.
Results
Intra-method variation was low for both methods (maximum CV 3.3% for Crisalix and 3.2% for VECTRA XT), with only nipple-to-nipple distance being statistically significant, marginally in favour of VECTRA. The mean inter-method differences were small but the limits of agreement (LoA) were wide for all parameters: best for sternal notch to nipple distance, mean difference (MD) -0.03cm and LoA 1.8 to -1.8cm; the widest LoA were for breast volume: MD 31.1cm3 and LoA 286.7 to -244.6cm3.
Conclusion
This is the first comparison of anthropometric distances and breast volume measured using the two most widely used 3D-SI systems, Crisalix and VECTRA XT. Intra-method variation is low but currently it would not be appropriate to use the two systems interchangeably due to the wide limits of agreement for all four parameters assessed.

Introduction
The use of three-dimensional surface imaging (3D-SI) was first described by Burke and Beard in 19671,2 to analyse facial structures. Modern-day 3D-SI is used as a marketing tool in aesthetic breast surgery. A 2016 survey of 1067 American plastic surgeons revealed that 15% were using 3D-SI technology in their practice3. Potential clients can view three-dimensional (3D) images of themselves and the surgeon can manipulate the images to demonstrate the expected appearances after breast augmentation or reduction, thereby enhancing communication and managing patient expectations4. Clinicians may also use 3D-SI to measure breast volume and anthropometric distances to improve pre-operative planning. In clinical research, changes in shape and position of the breast can be monitored post-operatively to assess stability over time after surgery or radiotherapy 4. Recent versions of the imaging systems have been developed which are smaller, more portable and cost effective 5-11 but have yet to be validated. There is some uptake of these systems among aesthetic plastic surgeons in the UK, but little amongst UK breast cancer surgeons.
Much of the work published to date has involved VECTRA XT (Canfield Sci, New Jersey, USA), a non-mobile system of six cameras which integrates the images into a 3D picture (figure 1). This can be measured 12-14 and adjusted to simulate future appearance 15 using the associated Mirror software (Canfield Sci, New Jersey, USA) and has been validated in breast cancer patients 16.

Figure 1. Image of person having breast imaging using the VECTRA XT (image reproduced with permission of Canfield Sci).
Crisalix (http://www.crisalix.com, Switzerland) is the first cloud-based 3D breast imaging system 17 (figure 2). It was designed as a patient education and marketing tool whereby the image of the patient’s torso can be manipulated to simulate a breast augmentation or reduction. Patients are imaged using a Structure Sensor (Occipital Inc, Boulder, CO, USA) mounted onto an iPad (Apple Inc., Cupertino, CA, USA). The Structure Sensor casts thousands of invisible infrared dots onto the object the user focuses on (in this case the patient’s torso). The sensor records the distance between each dot to construct a 3D geometric pattern as the user moves the iPad around the torso. Now, patients or their surgeons can upload three 2D photographs and the image is configured by the Crisalix web portal to create a 3D image, however, the infrared method is still recommended by Crisalix for greater accuracy.

Figure 2. Image of clinican taking 3D image using ipad and Structure Sensor which produces an image by the Crisalix web portal (image reproduced with permission of Crisalix).
Validation studies are necessary in order for 3D-SI measurements to become commonplace in everyday clinical practice13. To date, however, there are no studies comparing the validity, accuracy and reproducibility of the Crisalix imaging system with other more established 3D-SI systems18. In an adapted Delphi consensus study by Probst et al in 2005 seven desirable characteristics for 3D-SI imaging were identified. These included: i) to calculate breast volume accurately within 5%, ii) to detect a volume difference of 25cc or more, iii) measure distances with an accuracy of 5mm, iv) capable of capturing marks placed on significant breast points, v) cost less than £ 10 000, vi) fit in a footprint of <4m2 and vii) produce 3D images that are easily manipulated with minimal user experience.19 Both VECTRA and Crisalix meet several of these criteria and although both have been compared with mastectomy / MRI volumes 14, 20, 21, it is not known whether they can be used interchangeably because they have never been compared with each other. The aim of this study was therefore to compare the reproducibility and agreement between breast volume estimates and anthropometric measurements taken by the VECTRA XT and Crisalix 3D-SI systems.
Methods
Patient recruitment
Research Ethical Committee (REC) approval was obtained (ClinicalTrials.gov Identifier: NCT02304614) and an amendment was approved to permit comparison between VECTRA XT and Crisalix in a subset of women. The eligibility criteria for the main study were women aged ≥18 years who had undergone oncological breast-conserving treatment (BCT) for an invasive or in-situ carcinoma in our unit between one and six years before the start of the study. Patients with disease recurrence following BCT, as well as those with previous or subsequent surgery to the index or contralateral breast were excluded. Patients who were unable to stand for five minutes and follow instructions due to learning or physical disabilities or due to a language barrier were also excluded. Informed consent was obtained from all participants.
Patient measurements using VECTRA XT imaging system
The VECTRA XT system was calibrated daily according to the manufacturer’s instructions. Participants were imaged with their hands on their hips at the end of normal inspiration and the image was captured when the participant was deemed to be aligned by the software, approximately 1.5m from the cameras. The participant’s face was excluded from all images, so that only the torso was visible. Each participant was imaged three times with a break of one minute between each image. Markers were placed on each image at the sternal notch, nipple, lateral and medial limits of the breasts by the user. Thereafter, the calculation of anthropometric distances was automated (figure 3). A protocol was developed using the VAM software (Canfield Sci, New Jersey, USA) to measure breast volume and has been described elsewhere 16. The parameters (SN-N, N-N, breast width and breast volume) were calculated once per image.
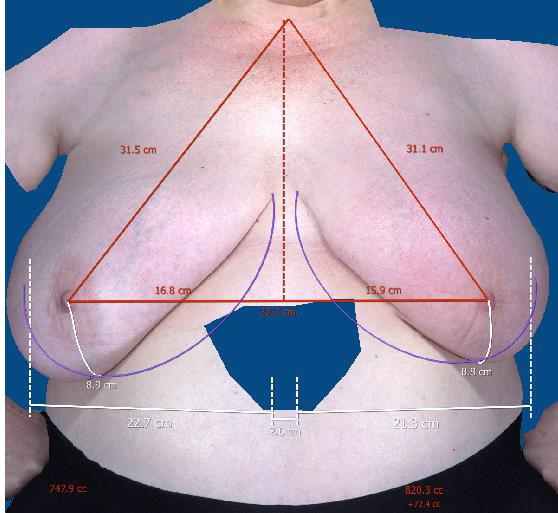
Figure 3. Image of participant’s torso with anthropometric measurements using VECTRA XT (Reproduced with permission from the participant)
Patient measurements using the Crisalix imaging system
The same participants were imaged using the Crisalix 3D-SI system on the same day and all by the same investigator (ROC). They stood in the middle of the medical photography room with their hand on hips. The 3D Structure Sensor was held 1m away from the participant and moved slowly up, down and side to side to fully capture the participant’s torso, in accordance with the manufacturer’s instructions. The software formed a 3D image and placed markers on the sternal notch, nipples and estimated a breast width and lasso around the base for volume analysis. Sternal notch and nipple markers cannot be moved by the user, but the width and lasso can be adjusted. Anthropometric and volume parameters were calculated (figure 4). Three images were captured and measured for each participant.
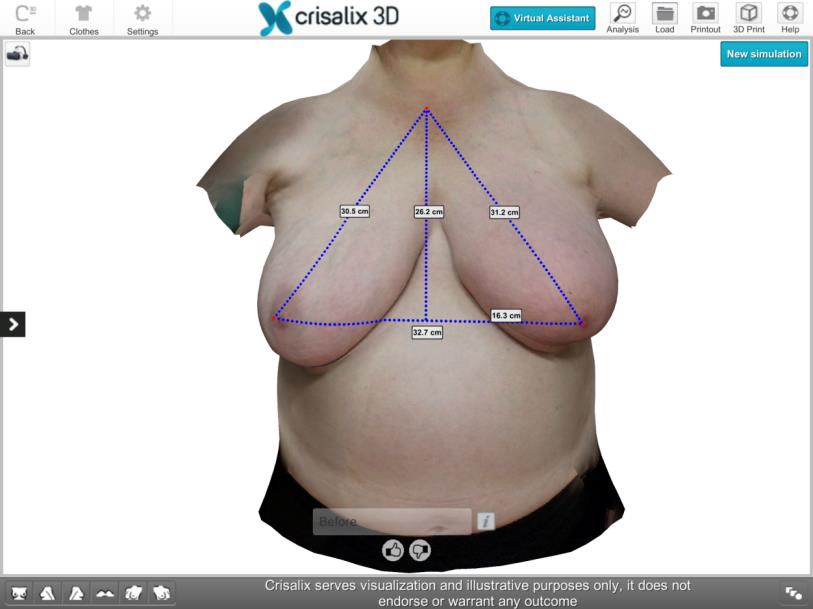
Figure 4. Image of the same participant as in figure 3 with anthropometric measurements using Crisalix. (Reproduced with permission from the participant)
Statistical analysis
Data were entered into an Excel spreadsheet (Microsoft Corp., Redmond, Washington) and subsequently analysed using SPSS statistical software (SPSS v22; SPSS, Inc., Chicago).
Intra-method and inter-method variability for in vivo 3D measurements
To assess intra-method variation, the mean of the standard deviations (SDs) for the 3 repeated measurements of each factor being assessed (SN-N, N-N, breast width and volume) were calculated. The mean coefficient of variation (CV = (SD / mean) %) was calculated for all of the parameters as an indication of the variation in each of the repeated measurements. Paired t-tests were used to compare the mean of the CVs with 5% significance levels.
Paired t-tests were also used to compare the mean of measurements taken with VECTRA XT and Crisalix (ie inter-method difference) with 5% significance levels. The agreement between the VECTRA XT and Crisalix measurements for each factor was calculated and graphically represented using Bland Altman plots 22. These display the difference between the means of the three measurements for each participant using the two imaging systems on the y axis (i.e. mean measurement VECTRA XT for patient A minus mean measurement Crisalix for patient A) as a function of the mean of the two imaging systems’ measurements on the x axis. The mean difference and ‘limits of agreement’ (mean difference +/- 1.96 times the standard deviation of the mean difference) were calculated.
Results
Patient recruitment
Of the 42 women who were contacted, 40 (95.2%) agreed to participate. Two (5%) women who agreed to participate did not attend. 38 women were imaged, but the first 3 women’s imaging data were not included in the study in order to reduce the impact of the learning curve on the Crisalix measurements. A further four women had blurred or deformed images using Crisalix and were excluded therefore, in total, images of 31 women were analysed.
Intra-method variation for VECTRA XT and Crisalix repeated measures
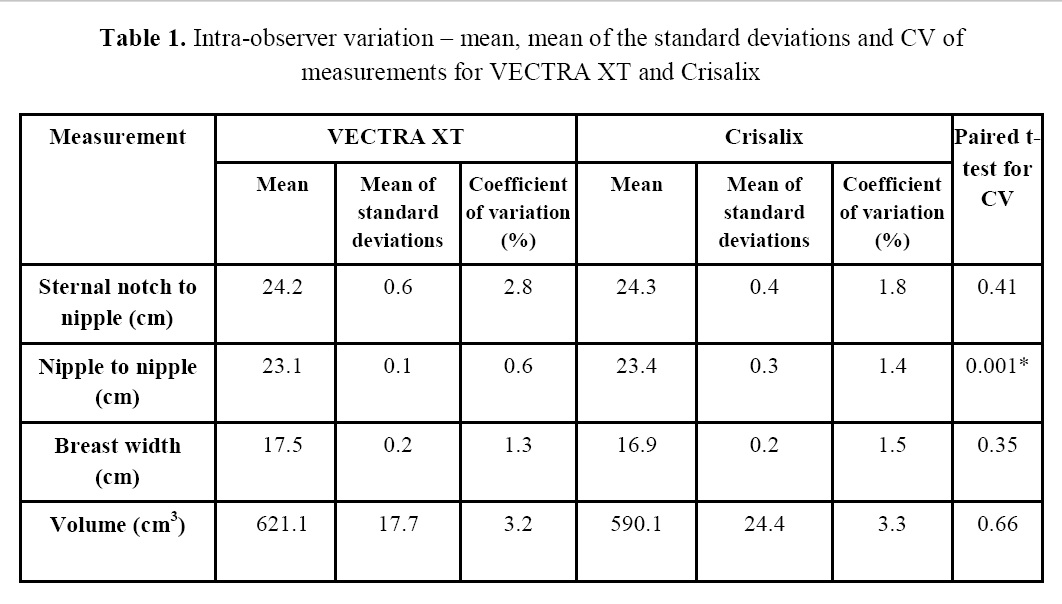
The mean, mean of the SDs, and CV for the three repeated measurements of SN-N, N-N, breast width and volume using the VECTRA XT and Crisalix systems are summarised in Table 1. Mean of SDs and CV were low for all parameters. The paired t-test for the CV showed that the only significant difference in variability for the VECTRA XT and Crisalix measurements was for nipple-to-nipple distance in favour of VECTRA XT (*).
Table 1. Intra-observer variation – mean, mean of the standard deviations and CV of measurements for VECTRA XT and Crisalix
Inter-method variation and Bland Altman agreement plots for VECTRA XT and Crisalix
The mean, mean difference, and limits of agreement for SN-N, N-N, breast width and volume are summarised in Table 2. There was a statistically significant difference between mean VECTRA XT and Crisalix measurements for nipple-to-nipple distance and breast width (*). Bland Altman plots are shown in Figures 5-8.
Table 2. Inter-method variation
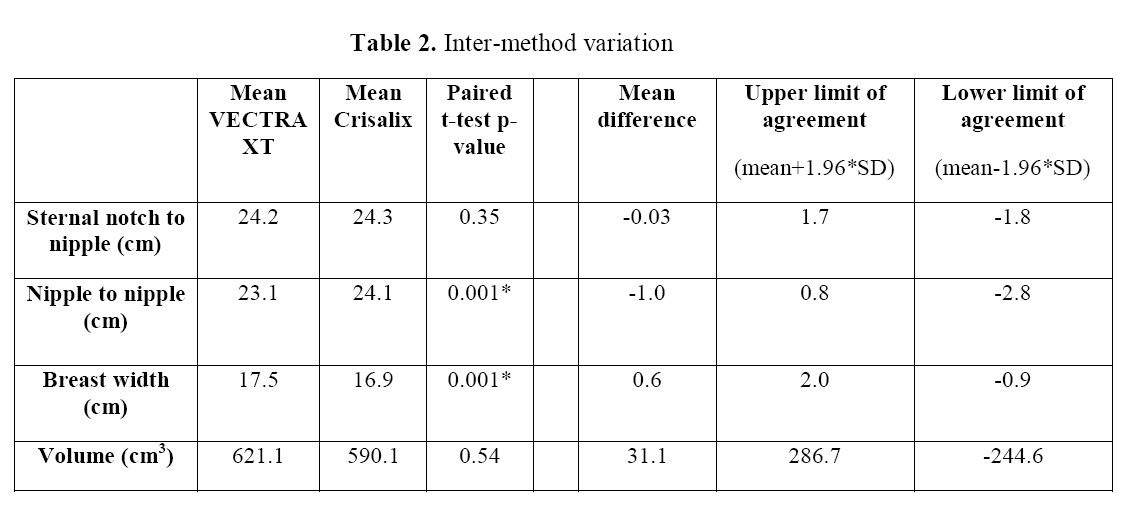
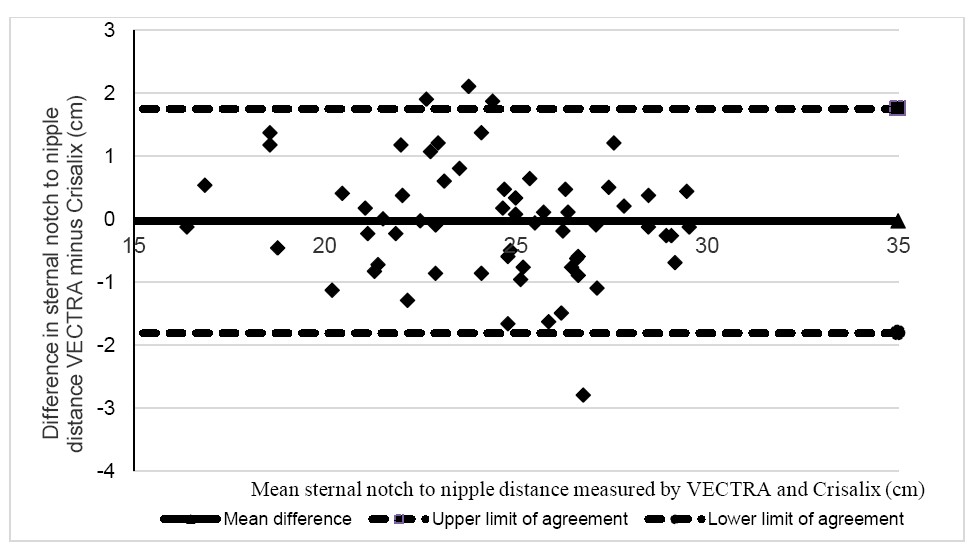
Figure 5. Bland Altman agreement plot for sternal notch to nipple (SN-N) distance
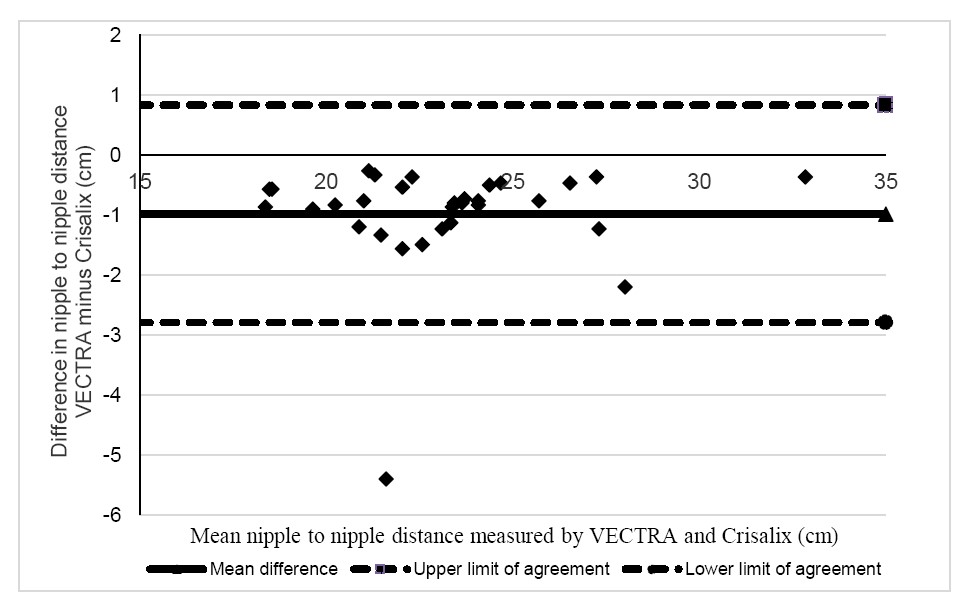
Figure 6. Bland Altman agreement plot for nipple to nipple distance
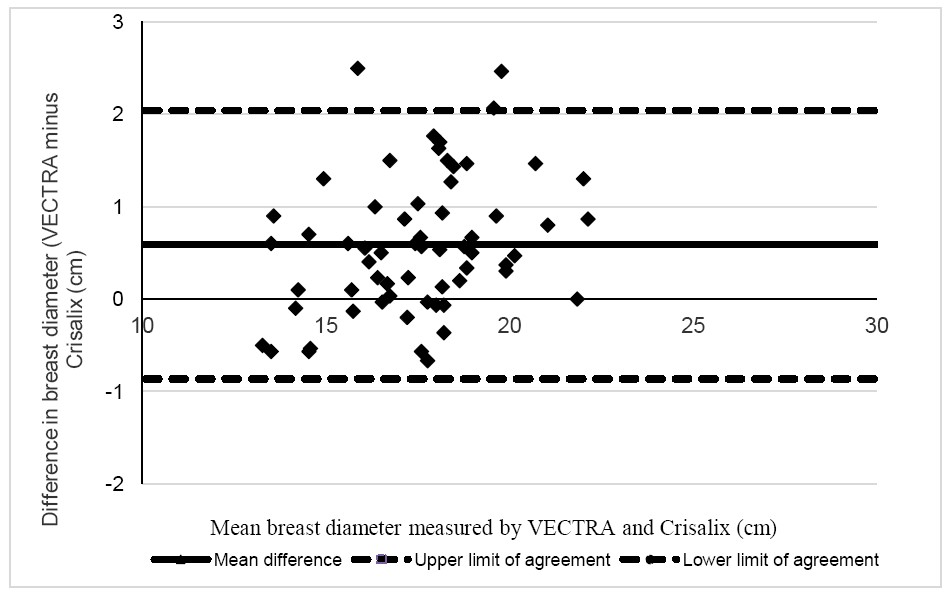
Figure 7. Bland Altman agreement plot for breast width
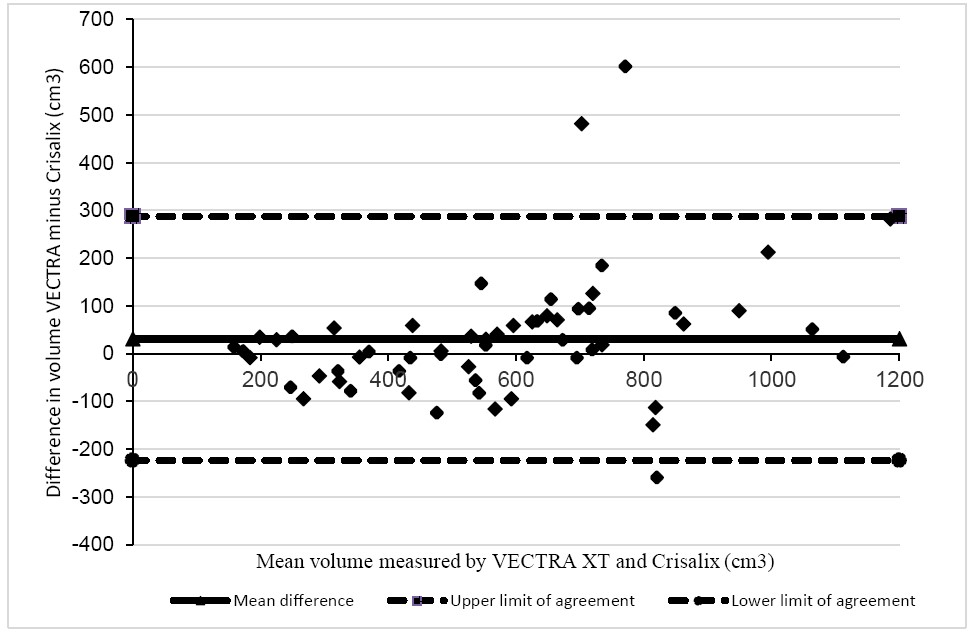
Figure 8. Bland Altman agreement plot for breast volume
For all four parameters, the mean difference was small but the limits of agreement were large. Often this was caused by one or two substantial outliers. In figures 5 and 6 (sternal notch to nipple and nipple to nipple distance) the outlier is the same patient. On review of her measurements, the left SN-N is consistently measured 2.8cm greater by Crisalix than by VECTRA and the nipple to nipple distance is measured 5.4cm greater by Crisalix. On inspection of the images, the right nipple marker is placed a little too lateral by Crisalix (and cannot be adjusted by the user). This would affect N-N but not left SN-N. This patient is also an outlier for volume with Crisalix calculating the left breast volume 250cm3 greater than VECTRA, see figure 9 below.
The two outliers in figure 7 have VECTRA XT measurement of width of 2.5cm greater than Crisalix. On review of their measurements and images, there is no clear reason as to why this should be.
The two outliers in figure 8 for which VECTRA measured volume substantially greater than Crisalix represent one participant whose abdominal wall slopes steeply postero-superiorly to antero-inferiorly (figure 9a). The case in which Crisalix measured breast volume substantially greater than VECTRA XT has an abdominal wall that slopes in the opposite way (slightly) (figure 9b). The interpolation of the posterior border of the breast is discussed in detail below.
Discussion
This study has shown that the variation of measurements taken by either Crisalix (3D sensor method) or VECTRA XT is small and either method can be used repeatedly with minimal natural variation. However, the limits of agreement between the two methods are wide such that the two cannot be used interchangeably.
Intra-method variation
The variation of measurements about the mean (i.e. CV) for both the VECTRA XT and Crisalix (3D sensor method) are small, with the largest variation being 3.3%. This concurs with previous work carried out by this group on intra- and inter- observer variation in measurements using VECTRA 16. The paired t-tests comparing the CVs demonstrated that there were no significant differences in variation of repeatability between the VECTRA XT and Crisalix measurements except for nipple to nipple distance, which was marginally in favour of the VECTRA XT measurements. Since this study was conducted, Crisalix have amended the software to allow users to enter a measured nipple to nipple distance which would calibrate the image and allow for images taken too close or far away from the patient. Of note, in the thumbnail images acquired during the scanning process, the outlier case in figures 5, 6, and 9 does not appear to be closer to the camera than other patients. Overall, therefore, this remains unexplained. VECTRA also has registration capabilities, but as we have previously demonstrated low intra-observer variation, these were not used.
Inter-method variation
When comparing VECTRA XT with Crisalix, there was a statistically significant difference in the means of nipple to nipple distance and breast width for the whole cohort, though the absolute difference in means (-1.0cm and 0.6cm respectively) would not be regarded as clinically significant and the values of the standard deviations were small. Nipple to nipple difference may be affected by the issues of scaling as mentioned above for the Crisalix system. Breast base width is notoriously difficult to measure, because of the difficulty in accurately identifying the lateral border of the breast, especially in overweight women. This may represent a difference in our patient population compared with the usual aesthetic augmentation population for which the systems have been developed.
More importantly, although the mean differences were small (for example Crisalix measured nipple to nipple distance on average 1cm larger than VECTRA), on a patient by patient basis the limits of agreement were wide (95% confidence this would lie within 0.8 to minus 2.8cm difference). Similarly, for volume, a mean difference of 31cm3 seems acceptable until one considers the 95% confidence interval from +286cm3 to -244cm3. This would clearly be regarded as a clinically important error. We therefore conclude that the two systems cannot be used interchangeably, for example in a multi-centre study.
The reasons for differences in linear measures have already been described. The two systems also have different methods for measuring volume: Crisalix applies a standard muscular shape as the posterior border of the breast. While this can be adjusted for individual patients, this adjustment was not made in this study to ensure uniformity. Conversely, the Mirror software associated with the VECTRA system interpolates the shape of the posterior border of the breast from the surrounding soft tissue anatomy. Both of these work well in slim augmentation candidates, however have their limitations in the generally older and heavier breast cancer population. Various studies have highlighted that the 3D-SI estimation of the posterior border of the breast (anterior chest wall) remains a particular challenge and this has a significant impact on the accuracy of breast volume measurement6, 23. A study by Göpper et al24 used CT images from patients in the general population to create a statistical shape model (SSM) by using principal component analysis (PCA) to factor in the chest wall in breast volume assessment. The authors found that the SSM-based estimation of breast volume was more accurate than the interpolation-based method.
Figure 9 shows the furthest outliers in figure 8, for breast volume, illustrating the musculature assumed by the Crisalix system and the trajectory of interpretation which might be taken by VECTRA software. It is important to note the blue line represents the authors’ estimation of possible interpolation of the posterior border of the breast by VECTRA leading to outlying poor agreement on volume between the two methods.
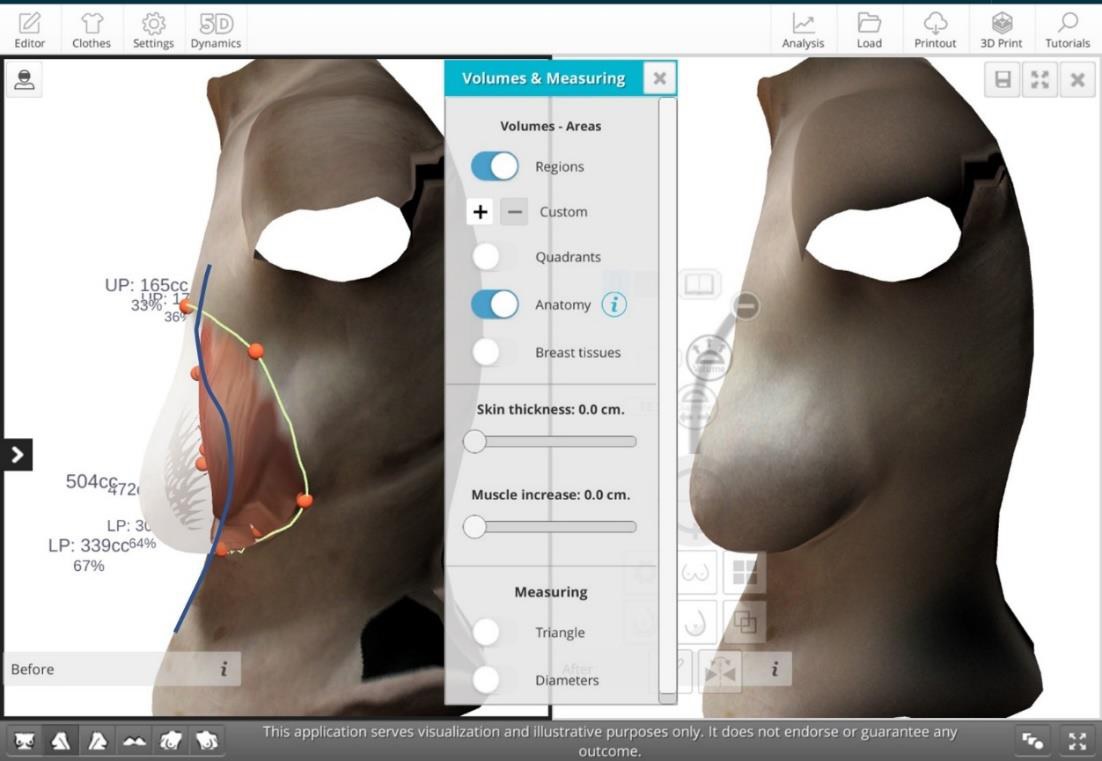
Figure 9a: Screenshot of image of a case with outlying datapoints for volume with VECTRA calculating greater than Crisalix. This demonstrates how, for this case, the VECTRA system will give a larger measurement for volume than the Crisalix system since extrapolation of the abdominal wall into the chest by VECTRA will lead to incorrect estimation of concavity. Conversely, the Crisalix musculature is illustrated in an unnaturally inferior position owing to the dislocation of the breast inferiorly on the chest wall with gravity.
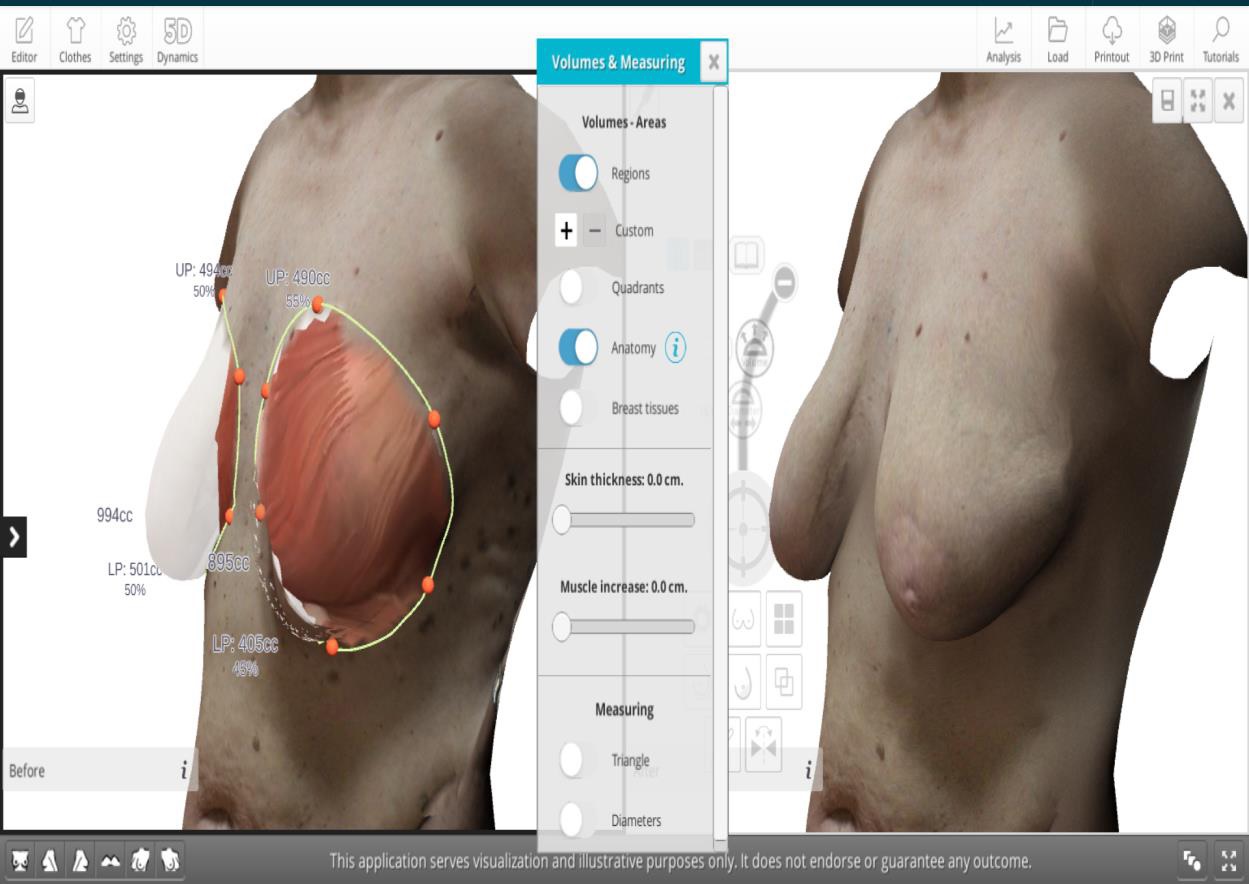
Figure 9b: Screenshot image of a case with outlying datapoints for volume with Crisalix calculating greater than VECTRA. Here the estimated VECTRA interpolation is shown in blue and the Crisalix musculature appears unnaturally recessed.
Other portable 3D-SI systems have been investigated, such as the Kinect recording system by Microsoft which is used in the gaming industry. The camera is designed to capture human motion and may be used in conjunction with a software program to produce an image and a depth map from which the volume can be calculated. Henseler et al 5 captured the images of nine silicone breast implants of different volumes four times and compared to the volume given by the manufacturer. The imaging system demonstrated slight over-estimation. However, the error did not exceed the 10% margin. Wheat et al 9 also compared breast measurements using a Microsoft Kinect 3D imaging system compared with manual measurements of straight line distance between two points on a mannequin. The mean difference was 1.9mm and excellent intra and inter-rater repeatability was demonstrated. While studies using phantoms or mannequins are informative, we have previously shown greater variation when measuring patients than plasticine phantoms 16.
Patete et al 7 compared a portable 3D-SI system to two established static systems. In this study they compared the image produced by the 3D imaging systems to that of a CT-derived reference model. The authors concluded that their portable prototype was accurate compared to two static cameras.
Further considerations
Portability and image capture: The Crisalix is far more portable and can be used anywhere with a stable internet connection. It takes approximately one minute to move the sensor around the participant to capture the image which may be challenging if the participant has poor balance or requires walking aids. The VECTRA XT is a static system and image capture is instantaneous, as the six digital cameras capture the digital photographs simultaneously. However, it takes up to 30 minutes to dismantle if required to move to another site.
Image storage: The Crisalix images are stored within the web portal and can be accessed on any computer that has downloaded the application. Secure Socket Layer (SSL) technology is used to encrypt data, to ensure that only authorised users can access the images. Any user would need institutional clinical and information governance permission to use it. The VECTRA XT images are stored on a computer hard drive and are only visible on that particular computer unless a network is set up and software installed onto other computers.
Image analysis: The Crisalix analysis is simple to use as only the medial and lateral mammary landmarks can be adjusted for volume and anthropometric measurements. However, a good internet connection is required for the volume calculations. It takes approximately one minute per breast to identify the region of interest and to obtain the volume calculation using the VECTRA XT system. Confident identification of the lateral mammary fold may be challenging in overweight or obese patients and this affects both systems. This issue is highlighted elsewhere in other studies which compared the VECTRA XT to traditional direct anthropometry25. With both systems it is possible to measure other straight-line distances which may be useful in surgical planning, for example, difference in height of the infra-mammary folds or the breast projection. It is also possible to superimpose images obtained over time to assess post-operative changes. These capabilities have not yet been validated. All studies comparing 3D-SI are dependent on the accuracy of their gold standard. It is worth noting that the repeatability of observers’ tape measurements has not been assessed, therefore both VECTRA XT and Crisalix may be more accurate than these.
Study limitations
Although the number of patients is small, we believe this is sufficient to illustrate the issues that would arise if using both 3D-SI systems interchangeably. Furthermore, software developments over time may already have reduced some of the inter-method disagreement and further improvements may yet be achieved.
Future directions
This study has compared the volumetric breast measurements using the VECTRA XT and Crisalix system and showed that these cannot be used interchangeably as the measurements vary significantly. Further studies are required to validate the Crisalix system for integrating 2D photographs to make a 3D images, to confirm its accuracy and objective reproducibility. Once validated, there may be scope to further investigate simulation of appearance after breast cancer surgery.
Conclusion
Each system shows good repeatability for all four parameters. While inter-method mean differences are small, it is not possible to use the Crisalix and VECTRA XT system interchangeably since the limits of agreement are wide.
Article Details
The Medical Research Archives grants authors the right to publish and reproduce the unrevised contribution in whole or in part at any time and in any form for any scholarly non-commercial purpose with the condition that all publications of the contribution include a full citation to the journal as published by the Medical Research Archives.
References
2. Burke P, Banks P, Beard L, Tee J, Hughes C. Stereophotographic measurement of change in facial soft tissue following surgery. BrJOral Sure. 1983;21(4):237-245.
3. Hidalgo D, Sinno S. Current Trends and Controversies in Breast Augmentation. Plast Reconstr Surg. 2016;137(4):1142-50.
4. O'Connell RL, Stevens RJ, Harris PA, Rusby JE. Review of three-dimensional (3D) surface imaging for oncoplastic, reconstructive and aesthetic breast surgery. Breast. Aug 2015;24(4):331-42. doi:10.1016/j.breast.2015.03.011
5. Henseler H, Kuznetsova A, Vogt P, Rosenhahn B. Validation of the Kinect device as a new portable imaging system for three-dimensional breast assessment. S1748-6815(13)00689-X pii ;10.1016/j.bjps.2013.12.025 doi. JPlastReconstrAesthetSurg. 2014;NOT IN FILE.
6. Hoeffelin H, Jacquemin D, Defaweux V, Nizet JL. A Methodological Evaluation of Volumetric Measurement Techniques including Three-Dimensional Imaging in Breast Surgery. 10.1155/2014/573249 doi. BiomedResInt. 2014;2014:573249. NOT IN FILE.
7. Patete P, Eder M, Raith S, Volf A, Kovacs L, Baroni G. Comparative assessment of 3D surface scanning systems in breast plastic and reconstructive surgery. 1553350612463443 pii ;10.1177/1553350612463443 doi. SurgInnov. 2013;20(5):509-515. NOT IN FILE.
8. Patete P, Riboldi M, Spadea MF, et al. Motion Compensation in Hand-held Laser Scanning for Surface Modeling in Plastic and Reconstructive Surgery. Annals of Biomedical Engineering. Sep 2009;37(9):1877-1885. doi:10.1007/s10439-009-9752-8
9. Wheat JS, Choppin S, Goyal A. Development and assessment of a Microsoft Kinect based system for imaging the breast in three dimensions. Medical Engineering & Physics. Jun 2014;36(6):732-738. doi:10.1016/j.medengphy.2013.12.018
10. Oliveira HP, Silva MD, Magalhaes A, Cardoso MJ, Cardoso JS. Is Kinect Depth Data Accurate for the Aesthetic Evaluation after Breast Cancer Surgeries? Pattern Recognition and Image Analysis, Ibpria 2013. 2013 2013;7887:261-268.
11. Stefanie T. L. Pöhlmann JH, Andrew I. Williamson, Jamie C. Sergeant, Alan Hufton,Ashu Gandhi, Christopher J. Taylor, Susan M. Astley. Breast Volume Measurement Using a Games Console Input Device, Breast Imaging. Breast Volume Measurement Using a Games Console Input Device, Breast Imaging. 2014;8539:666-678.
12. AR G, RL OC, PA B, et al. 3-Dimensional Objective Aesthetic Evaluation to Replace Panel Assessment After Breast Conserving Treatment. Breast Cancer2020.
13. Lin F, Hong W, Zeng L, Kong X, Feng W, Luo S. A Prospective Study of Breast Morphological Changes and the Correlative Factors After Periareolar Dual-Plane Augmentation Mammaplasty with Anatomic Implant. Aesthetic Plast Surg. Dec 2020;44(6):1965-1976. doi:10.1007/s00266-020-01665-7
14. Killaars RC, Preuβ MLG, de Vos NJP, et al. Clinical Assessment of Breast Volume: Can 3D Imaging Be the Gold Standard? Plast Reconstr Surg Glob Open. Nov 2020;8(11):e3236. doi:10.1097/gox.0000000000003236
15. Godden AR, Micha A, Pitches C, et al. 14. A Randomised Controlled Trial (RCT) of 3-Dimensional Simulation of Aesthetic Outcome in Breast Conserving Treatment (BCT). European Journal of Surgical Oncology. 2019/05/01/ 2019;45(5):880. doi:https://doi.org/10.1016/j.ejso.2019.01.200
16. O'Connell RL, Khabra K, Bamber JC, et al. Validation of the Vectra XT three-dimensional imaging system for measuring breast volume and symmetry following oncological reconstruction. Breast Cancer Res Treat. Jun 2018;doi:10.1007/s10549-018-4843-6
17. G E. Development and implementtion of a web-enabled 3D consultation breast augmentation surgery based on 3D-image reconstruction.
18. Chae M, Rozen W, Spychal R, Hunter-Smith D. Breast volumetric analysis for aesthetic planning in breast reconstruction: a literature review of techniques. Gland Surg. 2016;5(2):212-226.
19. Probst H, Choppin J, Wheat M, Harrison A. The development of a low cost 3D surface imaging system to measure breast volume: Defining minimum standards using an adapted Delphi consensus study. J Plast Reconstr Ästhet Surg. 2015;68(12):1170-1772.
20. Kim JH, Park JW, Woo KJ. Prediction of the Ideal Implant Size Using 3-Dimensional Healthy Breast Volume in Unilateral Direct-to-Implant Breast Reconstruction. Medicina (Kaunas). Sep 24 2020;56(10)doi:10.3390/medicina56100498
21. Wood KL, Zoghbi Y, Margulies IG, Ashikari AY, Jacobs J, Salzberg CA. Is the Vectra 3D Imaging System a Reliable Tool for Predicting Breast Mass? Ann Plast Surg. Jul 2020;85(S1 Suppl 1):S109-s113. doi:10.1097/sap.0000000000002333
22. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. Feb 1986;1(8476):307-10.
23. Lee W, Kim M, Lew D, Song S, Lee D. Three-Dimensional Surface Imaging is an Effective Tool for Measuring Breast Volume: A Validation Study. Arch Plast Surg. 2016;43:430-437.
24. Göpper M, Neubauer J, Kalash Z, Stark G, Simunovic F. Improved accuracy of breast volume calculation from 3D surface imaging data using statistical shape models. PLoS ONE. 2020;15(11):e0233586.
25. Steen K, Isaac K, Murphy B, Beber B, Brown M. Three-Dimensional Imaging and Breast Measurements: How Predictable Are We? Aesthet Surg. 2018;38(6):616-22.