
Cervical Schwannoma of the Vagus Nerve: Systematic Review and Two Illustrative Cases
Main Article Content
Abstract
Background: Cervical schwannoma is a rare and benign tumor exclusively developed from the cell of Schwann that rarely involve the vagus nerve.
Methods: We have conducted a retrospective review with strategy of the consulted references and database included articles published in Portuguese, English and French in PUBMED, MEDLINE, EMBASE, LILACS and SciELO, since 1936 until the present day, associated with a description of two illustrative cases. Both patients presented with a history of painless palpable mass in the cervical region.
Results: About 160 cases has been described in literature. Most cases of manifest between the third and sixth decades of the patient's life as a slow growing firm, painless mass in the lateral neck. Imaging is essential to management. Histopathological examination can reveals encapsulated, biphasic spindle cell neoplasia. The best choice of treatment for this type of tumor is complete surgical removal with preservation of the vagus nerve by means of intracapsular resection. In both ilustrative cases the lesions were diagnosed by means of imaging studies and were totally ressected. Surgical findings and histopathology confirmed the diagnosis of vagus nerve schwannoma. There was no recurrence at five years of follow-up. In one case there was disphonya that solved within six months after the surgery.
Conclusion: Vagus nerve schwannomas are rare benign tumors. The enucleation technique is used to obtain the most functional preservation and complete excision without permanent deficit is possible even with the occurrence of large lesions.

Introduction
Schwannoma is a benign tumor exclusively developed from the cells of Schwann surrounding nerve fibers in the peripheral nervous system. These lesions may occur in the cervical region by up to 25% of cases and should be suspected in the presence of an isola ted lateral cervical mass. Surgical treatment is the best choice, especially with a growing mass. The preservation of nerve function with complete resection is often possible since tumor develops extrinsically and displaces the remaining fascicles. The pur pose of this report is present a systematic review associated with a description of two illustrative cases of this uncommon disease.
Methods
The search strategy of the consulted references and database included articles published in Portuguese, English an d French in PUBMED, MEDLINE, EMBASE, LILACS and SciELO. They were evaluated review articles, systematic reviews and meta - analyzes. The keywords used to find such results were: vagus nerve, schwannoma, peripheral nerve tumor, cervical vagus nerve. Papers ex cluded with cervical sympathetic chain schwannoma, jugular forame schwannoma, glossopharyngeal schwannoma, middle mediastinum, malignant cases, intrathoracic vagal nerve schwannoma, retroperitoneal schwannoma of the vagus nerve and papers containing vagus and other schwannomas without distinction.
This paper presents description of two illustrative cases of this disease.
Illustrative cases
Case 1
L.C.M.S., 34- year- old male, perceived the tumor in the right cervical region two years ago. There has been rapid growth of the lesion.
The physical exam revealed a painless nodule upon palpation in right cervical region, firm, insensitive and mobile. There was no associated dysphagia, dysphonia or neurologic deficit .
Biopsy by fine - needle aspiration cytology was performed and the histological findings were compatible with schwannoma.
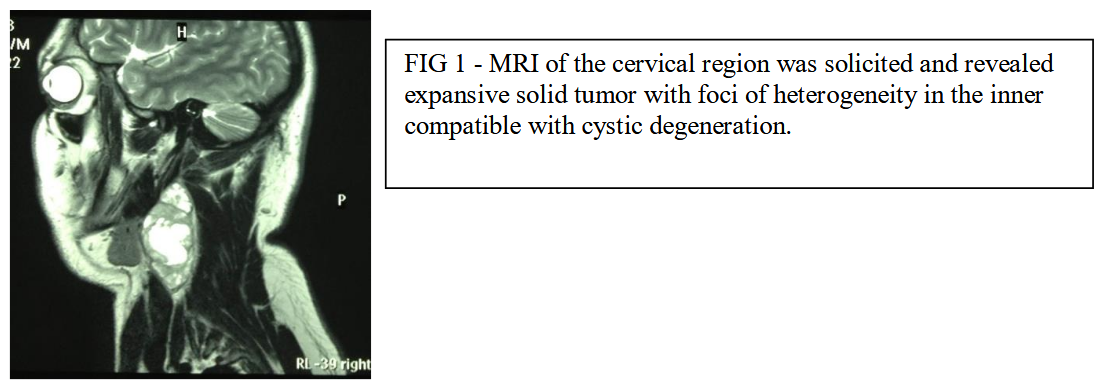
Nuclear magnetic resonance imaging (MRI) of the cervical region was solicited and revealed expansive tumor measuring 7,7 x 3,4 x 3,0 solid with foci of heterogeneity in the inner compatible with cystic degeneration.
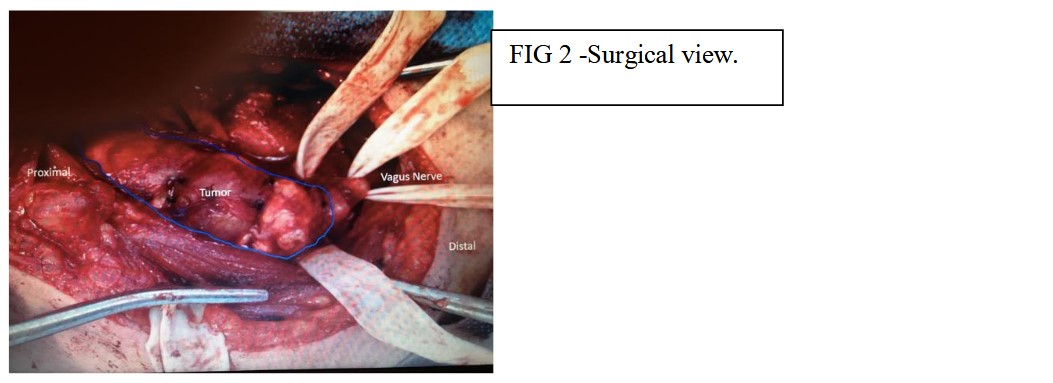
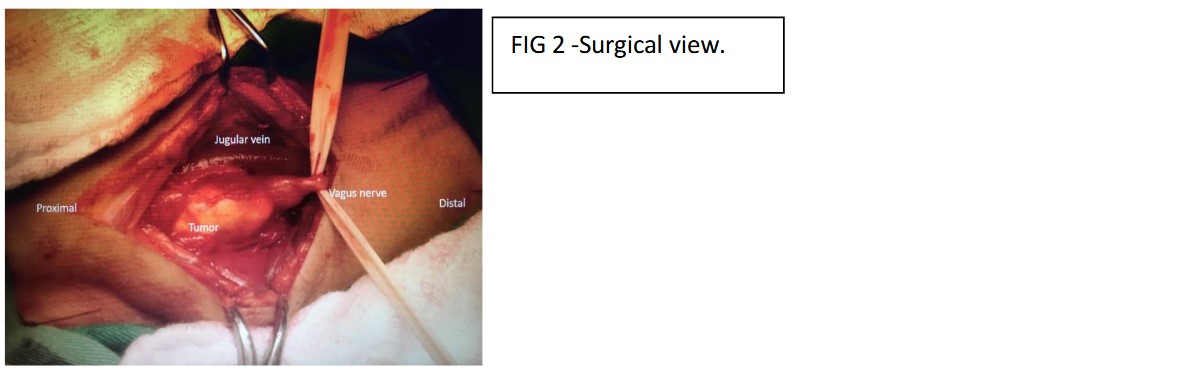
In June 2 013, L.C.M.S. underwent microsurgery in which the lesion was totally resected by intracapsular enucleation and the nerve was preserved. Surgical exploration found a heterogeneous 8.0 x 4.0 cm mass causing anterior displacement of the internal jugular vein and vagus nerve and medial displacement of the carotid vessels, diagnosis pointed to benign schwannoma.
The immediate postoperative coursed with dysphonia.
Case 2
R.M.N.C., 35 - year - old female, perceived the tumor in the right cervical region. The physical exam revealed a painless nodule upon palpation in right cervical region, firm, mobile in the horizontal but not in vertical direction. There was no neurologic deficit .
This case was not underwent to biopsy fine - needle aspiration cytology.
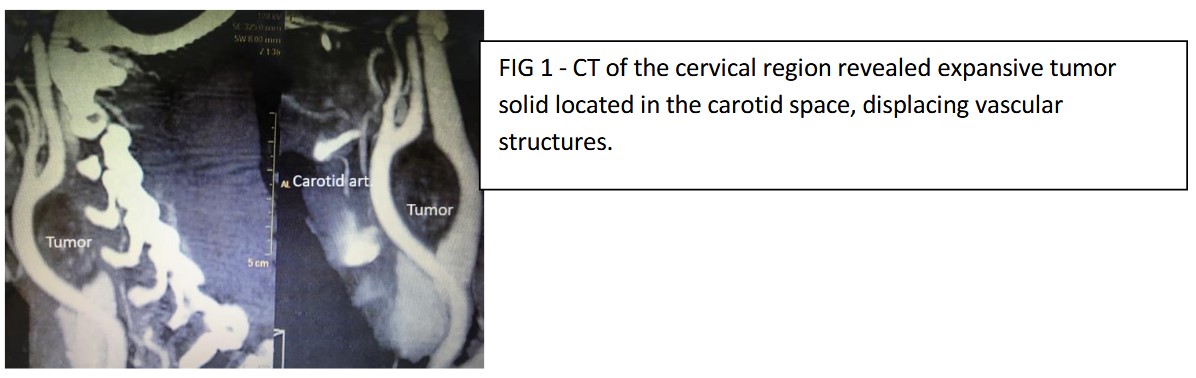
Computerized tomography showed a well - defined mass with anterior displacement of the common and internal carotid artery ( 4,0 x 2,0 cm) solid, located in the carotid space, displacing previously vascular structures.
Using a skin crease incision, surgical exploration found displacement of the external jugular, a well encapsulated tumor arising from the vagus nerve was noted. Tumor was enucleated with sparing of the nerve, the lesion was totally resected and the nerve preserved.
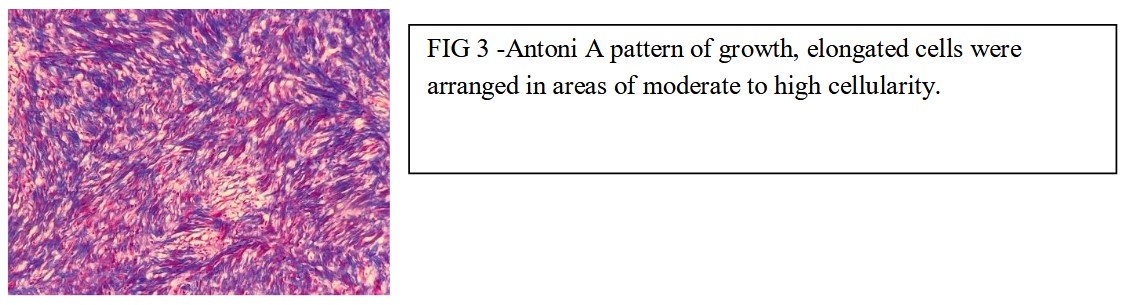
In the immediate postoperative there was no neurological deficit. Histopathology showed Antoni A pallisading nucleus and verruca bodies suggestive of schwanoma.
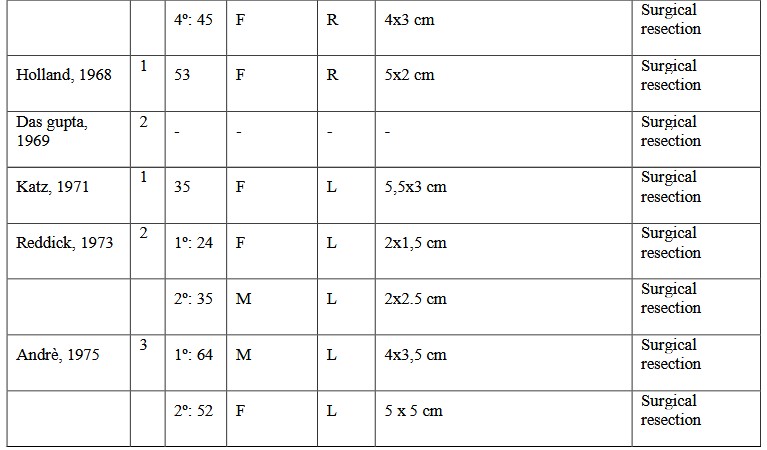
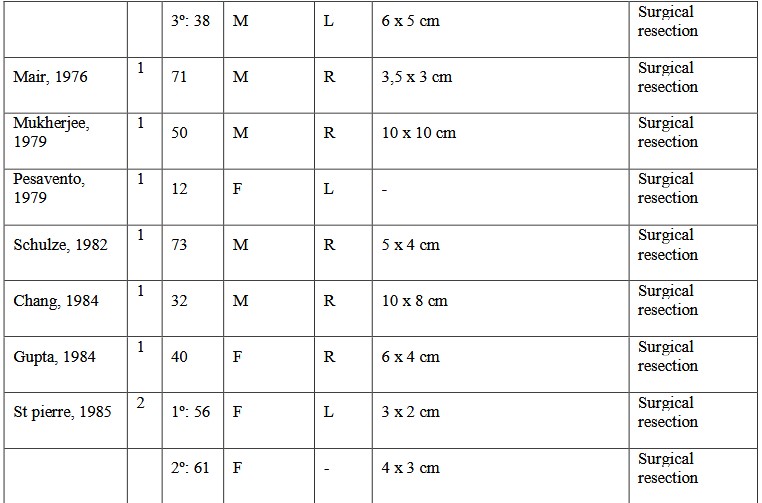
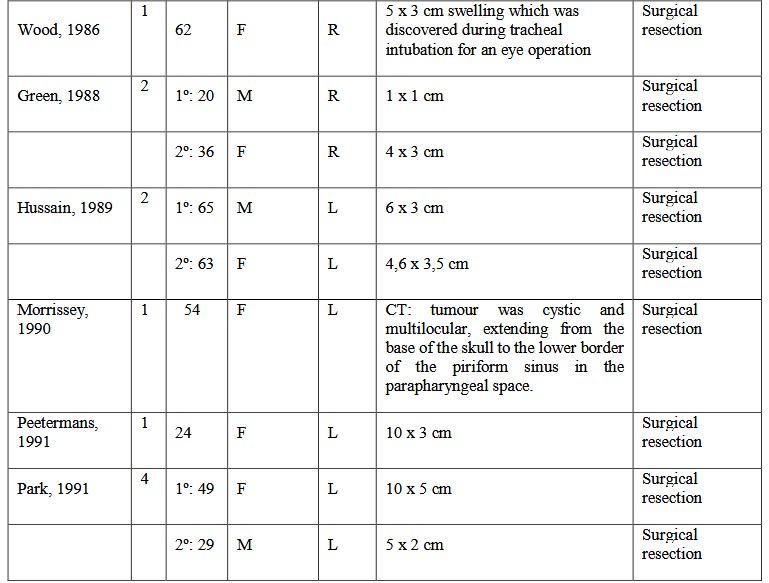
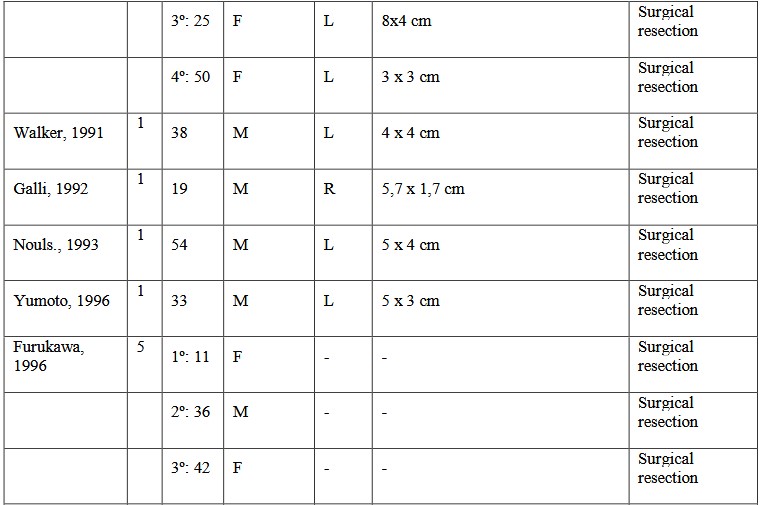
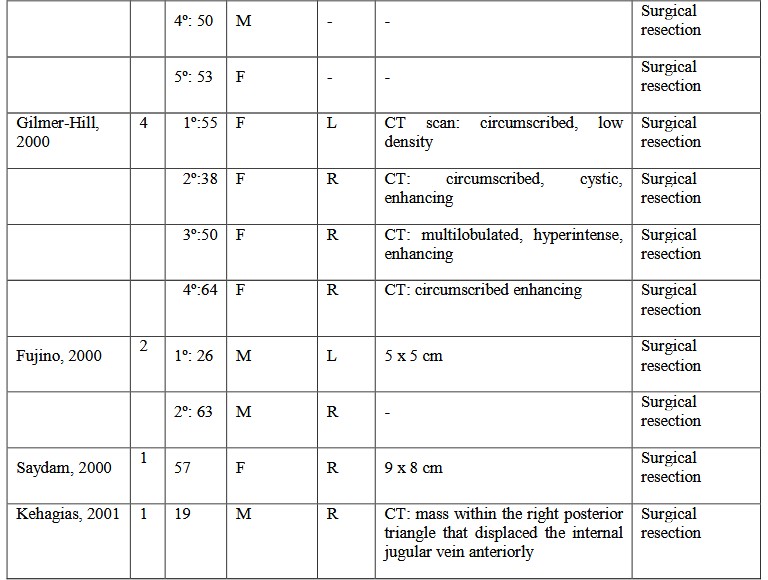
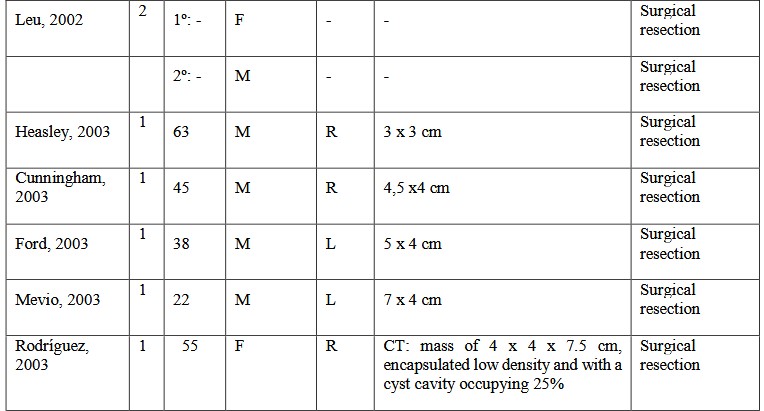
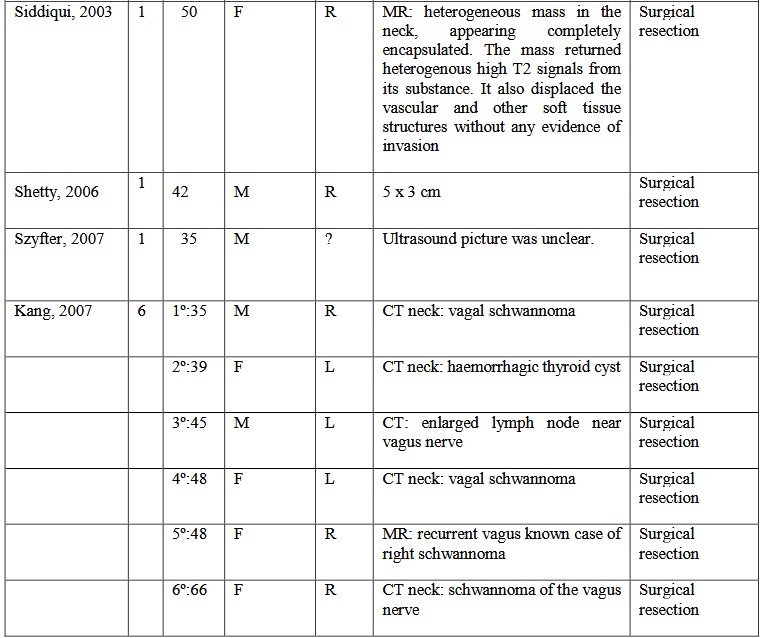
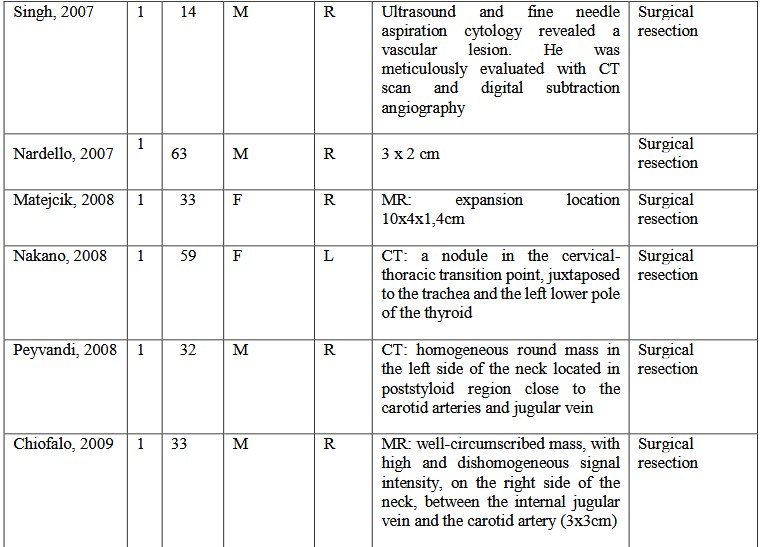
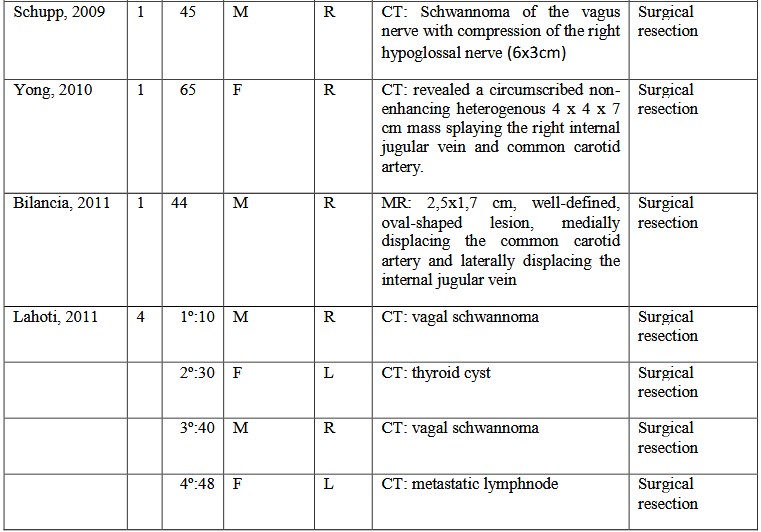
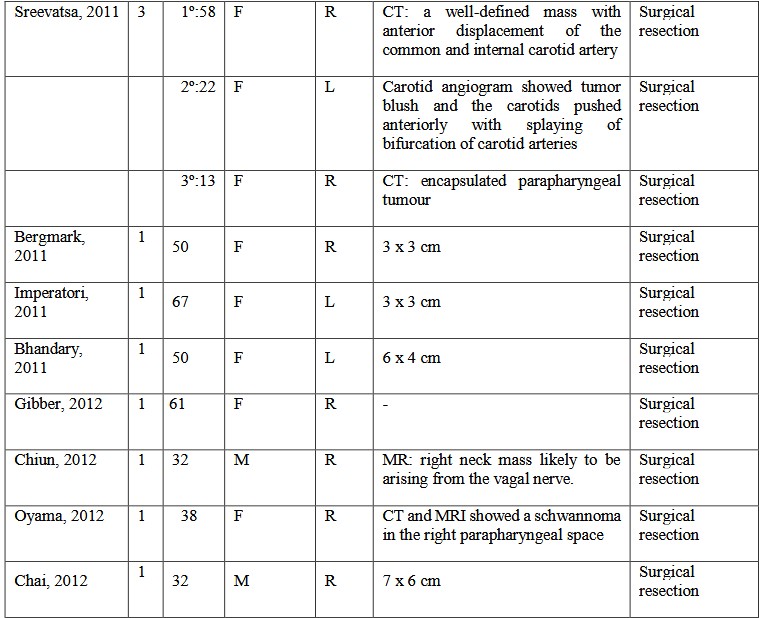
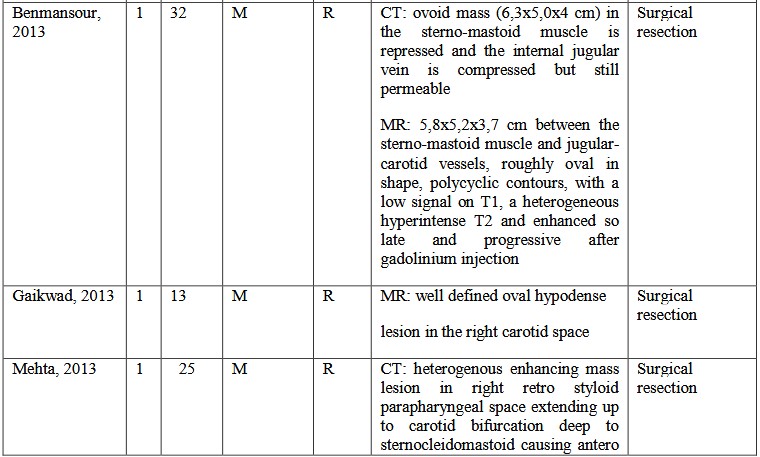
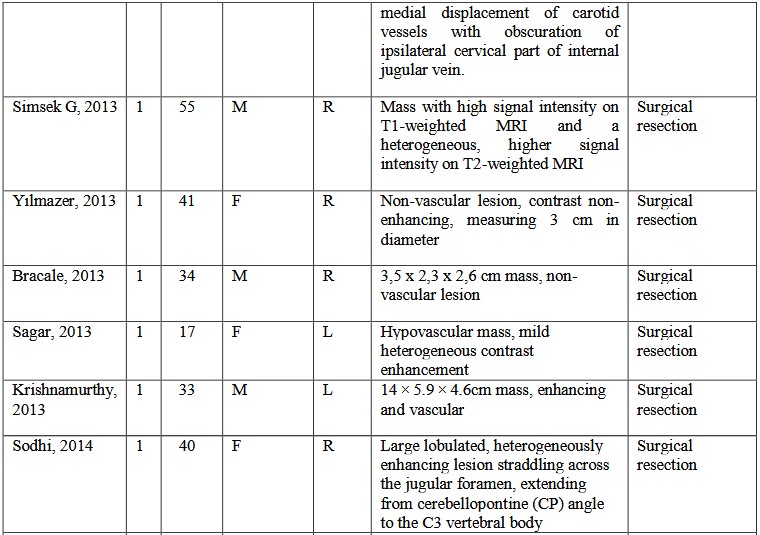
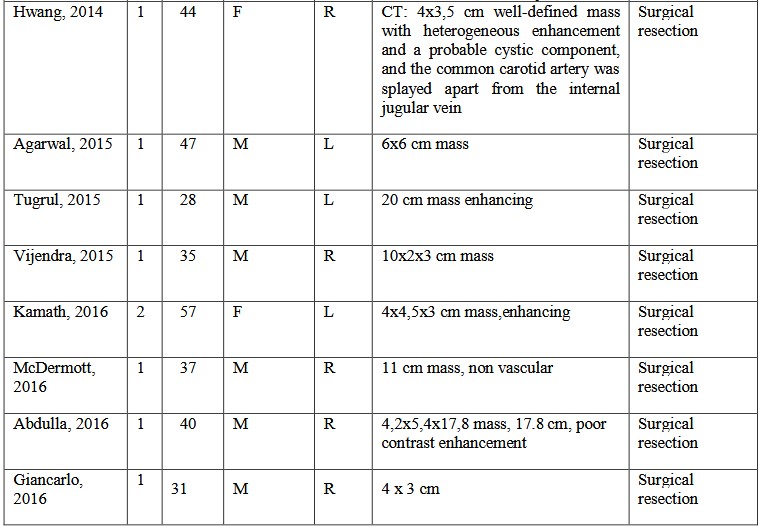
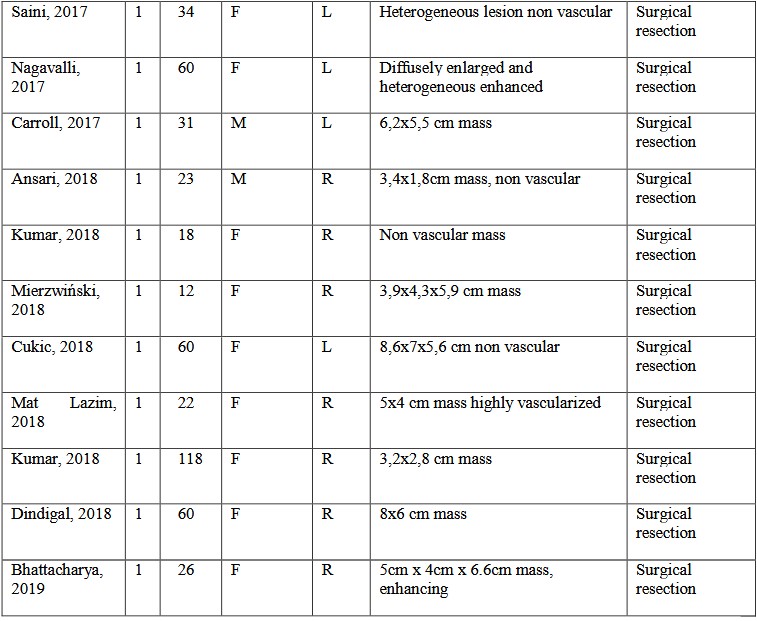
Table
Discussion
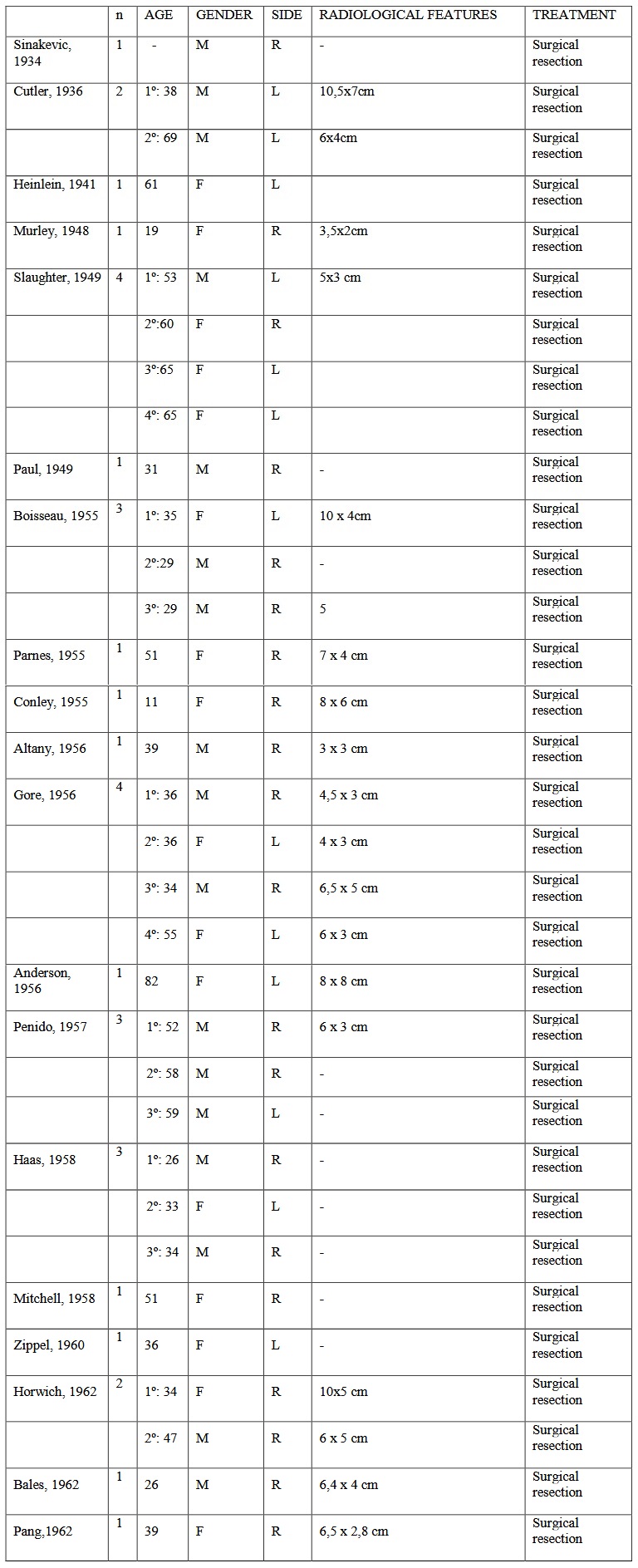
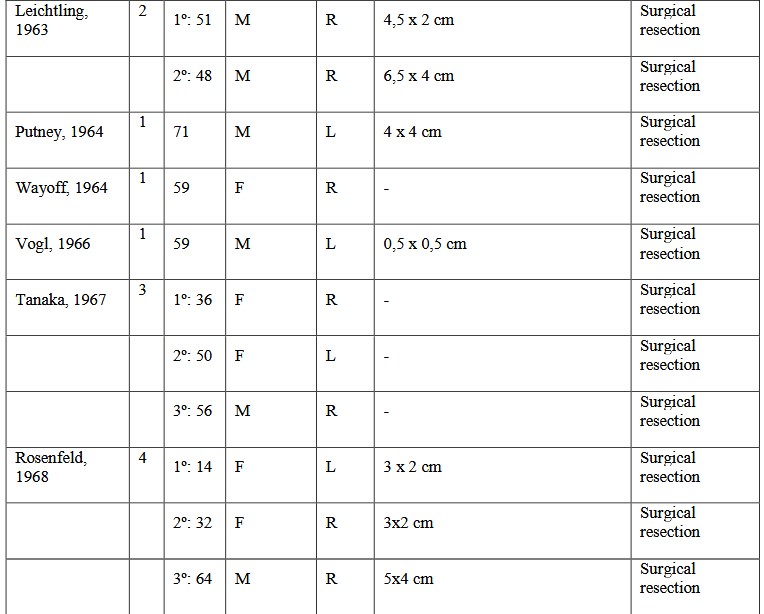
Cervical vagus schwannoma was first reported by Ritter in 1899 (apud Yumoto et al). 110 Since that, 160 cases has been described in the literature. This tumor most often presents as a slow growing asymptomatic solitary neck mass. 61
Most cases of cervical schwannomas manifest between the third and sixth decades of the patient’s life as a slo w growing firm, painless mass in the lateral neck. Hoarseness, pain, or cough may be the presenting complaints. The tumor usually displace the carotid arteries anteriorly and medially, jugular vein laterally and posteriorly. Generally, these lesions are mo vable transversely but not vertically. 61 Those typical features were found in our two cases.
Pre - operative diagnosis of schwannoma is difficult because many vagal schwannomas do not present with neurological deficits and several differential diagnoses for tumour of the neck may be considered, including paraganglioma, branchial cleft cyst, malignant lymphoma, metastatic cervical lymphadenopathy and neurofibromas. 110 Topographic features may be helpful in distinguishing origin nerve at initial presentation: the vagal schwannomas should be displaced between the internal jugular vein laterally and the carotid artery medially, where as schwannomas from the cervical sympathetic chain displace both the carotid artery and jugular vein without separating them . 43 In our case 2, the tumor displaced the internal jugular vein laterally and anteriorly.
Imaging is essential to management. CT and nuclear MRI determine tumor size, extension and relation to the internal and external carotids. 109 The MRI is considered typ ical when the mass appears as a well - circumscribed tumor lying between the internal jugular vein and the carotid artery. 48 Radiological aspects in CT can show well defined mass compressed the internal jugular vein or internal carotid 19 or rare presentation with heterogenous enhancing mass lesion in right retro styloid parapharyngeal space extending up to carotid bifurcation deep to sternocleidomastoid causing antero medial displacement of carotid vessels with obscuration of ipsilateral cervical part of inte rnal jugular vein. 61 MRI can show more details: dimensions, polycyclic contours, low signal on T1, a heterogeneous hyperintense T2 and enhanced so late and progressive after gadolinium injection among other things. 19
The use of fine - needle aspiration an d cytology is still controversial; the majority of authors does not recommend open or needle biopsy for these masses. 68 In this study, only one case was biopsied.
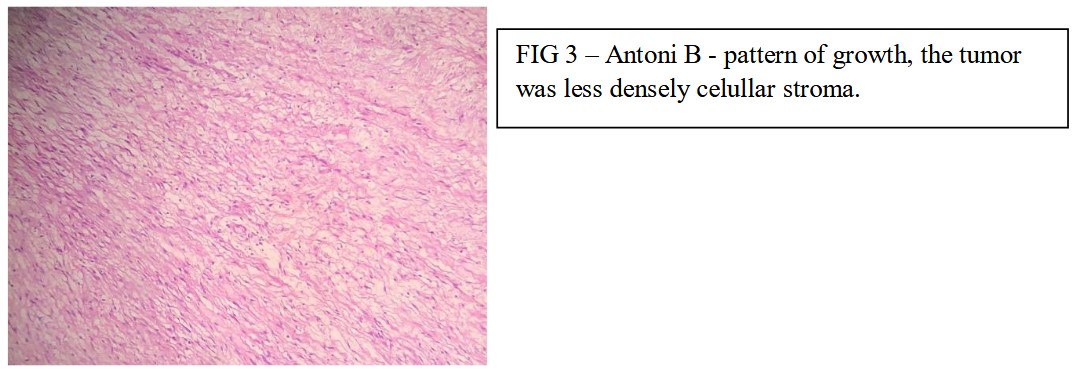
Histopathological examination can reveals encapsulated, biphasic spindle cell neoplasia. There are more cellular areas (Antoni A) where nuclei are sometimes palisaded around collagenized bands forming structures known as Verocay bodies, as well as collagen globules, often found in sheath - derived neoplasms peripheral nerve neural disease. In other less cellular and loose stromal areas (Antoni B) cystic degeneration is often observed and hyalinized vessels. Fibrous capsule evidenced by Masson's trichrome staining 98
In particular, cystic vagal schwannomas originating from the cervical vagus nerve are extremely rare 68 limited to 160 cases in the literature.
The best choice of treatment for this type of tumor is complete surgical removal with preservation of th e vagus nerve by means of intracapsular resection. 79 The two patients here reported underwent surgery with intracapsular resection.
Nerve palsy is a common complication of the vagal schwannoma removal, but in many cases it recovers spontaneously when the neural integrity is preserved. 79 In our case 1, there was vocal cord palsy, which fully recovered in six months after the operation. In case 2 there was no vocal cord palsy or another complication. Horner’s syndrome is also a usual postoperative complicati on 111 absent in our cases.
Conclusion
Vagus nerve schwannoma is a rare benign tumor to be suspected in the presence of an isolated lateral cervical mass. Imaging studies are essential to the management.
Surgical treatment is the best choice, especially if the tumor is growing. The conservation of the original nerve is often possible
Article Details
The Medical Research Archives grants authors the right to publish and reproduce the unrevised contribution in whole or in part at any time and in any form for any scholarly non-commercial purpose with the condition that all publications of the contribution include a full citation to the journal as published by the Medical Research Archives.
References
2. Cutler EC, Gross RE. The surgical treatment of tumors of the peripheral nerves. Ann Surg. 1936; 104(3): 436-52.
3. Heinlein, R. 1941 quoted by Kleinsasser O. On neurinomas oft he cranial nerves and cervical sympathetic nervous system. HNO. 1964; 12: 308-16.
4. Murley RS. A case of neurinoma of the vagus nerve in the neck. Br J Surg. 1948; 36(141): 101-3.
5. Slaughter DP, Depeyster FA. Pharyngeal neurilemmomas of cranial nerve origin; medical displacement of the internal carotid artery as a diagnostic sign. Arch Surg. 1949; 59(3): 386-97.
6. Paul M. Nerve sheath tumours of the vagus nerve in the neck. Aust N Z J Surg. 1949; 19(1): 34-7.
7. Boisseau M. Tumors of the pneumogastric nerve in its cervical course. Rev Laryngol Otol Rhinol (Bord). 1955; 76(9-10): 539-600.
8. Parnes IH. Tumor of the vagus nerve. Surgery. 1955; 37(6):955-8.
9. Conley JJ. Neurogenous tumors in the neck. AMA Arch Otolaryngol. 1955; 61(2): 167-80.
10. Altany FE, Pickrell KL. Neurilemomas of the vagus nerve in the neck. AMA Arch Surg. 1956; 73(5): 793-800.
11. Gore DO, Rankow R, Hanford JM. Parapharyngeal neurilemmoma. Surg Gynecol Obstet. 1956; 103(2): 193-201.
12. Anderson R, Harrison B Jr. Neurilemomas of the lateral region of the neck. Cleve Clin Q. 1956; 23(4): 274-9.
13. Penido JR, Dodge HW, Clagett OT, et al. Tumors of the vagus nerve. Proc Staff Meet Mayo Clin. 1957; 32(10): 239-49.
14. Haas E. Treatment of vagus neurinoma. Arch Ohren Nasen Kehlkopfheilkd. 1958; 173(2): 289-95.
15. Mitchell JF. Extracranial neurilemmoma of the vagus. J Laryngol Otol. 1958; 72(2): 166-71.
16. Zippel, R. Differential diagnostic data on neurogenic solitary tumors of the mesopharynx. Arch Ohren Nasen Kehlkopfheilkd. 1960; 176: 563-569.
17. Horwich M, Hawe P. Neurilemmoma of the vagus nerve in the neck with report of two cases. Br J Surg. 1962; 49: 443-6.
18. Bales HW, Raines M. Neurilemmoma of the vagus nerve. N Y State J Med. 1962; 62: 105-7.
19. Pang LQ. Schwannoma of the cervical portion of the vagus nerve. Case report. Ann Otol Rhinol Laryngol. 1962; 71: 489-97.
20. Leichtling JJ, Lesnick GJ, Garlock JH. Neurliemmomas of vagus nerve in the neck. A significant diagnostic sign. JAMA. 1963; 183: 143-5.
21. Putney FJ, Moran JJ, Thomas GK. Neurogenic Tumors Of The Head And Neck. Laryngoscope.1964; 74: 1037-59.
22. Wayoff M, Bemol P. Neurinoma Of The Pneumogastric Nerve At The Level Of The Neck. Ann Otolaryngol Chir Cervicofac. 1964; 81: 516-7
23. Vogl A. Neurinoma of the vagus nerve. (1966) Zentralbl Chir. 1966; 91(50): 1881-3.
24. Tanaka T, Iwabuchi T, Suzuki J, et al. 3 surgical cases of schwannoma of the vagus nerve located in the neck. No To Shinkei. 1967; 19(10): 983-8.
25. Rosenfeld L, Graves HJR, Lawrence, R. Annals of surgery. 1968; 167: 847.
26. Holland GW. Neurilemmoma of the vagus nerve in the neck. Aust N Z J Surg. 1968; 38(2): 146-8.
27. Das Gupta TK, Brasfield RD, Strong EW, et al. Benign solitary Schwannomas (neurilemomas). Cancer. 1969; 24(2): 355-66
28. Katz AD, Passy V, Kaplan L. Neurogenous neoplasms of major nerves of face and neck. Arch Surg. 1971; 103(1): 51-6.
29. Reddick LP, Myers RT. Neurilemmoma of the cervical portion of the vagus nerve. A collec.tive review and two case reports. Am J Surg. 1973; 125(6): 744-7.
30. Andrè P, Laccourreye H, Haguet JF. Annales d'otolaryngologie et chirurgie cervico-faciale. 1975; 92, 345.
31. Mair IW, Marhaug GO, Stalsberg H. Solitary schwannoma of the cervical vagus nerve. ORL J Otorhinolaryngol Relat Spec. 1976; 38(6): 344-9.
32. Mukherjee DK. Neurilemmoma of the vagus nerve: a case report. J Laryngol Otol. 1970; 93(2): 187-92.
33. Pesavento G, Ferlito A, Recher G. Benign solitary schwannoma of the cervical vagus nerve. A case report with a review of the literature. J Laryngol Otol. 1979 93(3): 307-16.
34. Schulze S, Krogdahl A. Schwannoma of the vagus nerve. Acta Chir Scand. 1982; 148(7): 627-8.
35. Chang SC, Schi YM. Neurilemmoma of the vagus nerve. A case report and brief literature review. Laryngoscope. 2004; 94(7):946-9.
36. Gupta SC, Mehdiretta NK. Neurilemmoma of vagus nerve in the neck. J Indian Med Assoc. 1984; 82(1): 19-20.
37. St Pierre S, Theriault R, Leclerc JE. Schwannomas of the vagus nerve in the head and neck. J Otolaryngol. 1985; 14(3): 167-70.
38. Wood BM, Mcneil WT. Schwannoma of the vagus nerve. Anaesthesia. 1986; 41(11): 1130-1132.
39. Green JD, Olsen KD, DeSanto LW, et al. Neoplasms of the vagus nerve. Laryngoscope. 1988; 98(6 pt 1): 648-54.
40. Hussain SSM, Watson MG, Pahor AL. Neurilemmoma of the vagus nerve in the neck. Ear Nose and Throat Journal. 1989; 68(1): 52-6.
41. Morrissey MS, Sellars SL.Vagal nerve schwannoma-a new diagnostic sign. Postgrad Med J. 1990; 66(771):42-3.
42. Peetermans JF, Van de Heyning PH, Parizel PM, et al. Neurofibroma of the vagus nerve in the head and neck: a case report. Head Neck. 1991; 13(1): 56-61.
43. Park CS, Suh KW, Kim CK. Neurilemmomas of the cervical vagus nerve. Head Neck. 1991; 13(5): 439-41.
44. Walker WA, Maguire FE. Vagal schwannoma. Ann Thorac Surg. 1991; 52(6): 1370-1.
45. Galli J, Almadori G, Paludetti G, et al. Plexiform neuro fibroma of the cervical portion of the vagus nerve. J of Laryngol Otol. 1992; 106(7): 643-648.
46. Nouls P, Hassid S, Choufani G, et al. Neurinoma of the cervical vagus nerve. A propos of a case-literature review. Acta Otorhinolaryngol Belg. 1993; 47(4): 449-54.
47. Yumoto E, Nakamura K, Mori T, et al. Parapharyngeal vagal neurilemmoma extending to the jugular foramen. J Laryngol Otol. 1996; 110(5): 485-9.
48. Furukawa M, Furukawa MK, Katoh K, et al. Differentiation between schwannoma of the vagus nerve and schwannoma of the cervical sympathetic chain by imaging diagnosis. Laryngoscope. 1996; 106(12 pt 1): 1548-52.
49. Gilmer-Hill HS, Kline DG. Neurogenic tumors of the cervical vagus nerve: report of four cases and review of the literature. Neurosurgery. 2000; 46(6): 1498-1503.
50. Fujino K, Shinohara K, Aoki M, et al. Intracapsular enucleation of vagus nerve-originated tumors for preservation of neural function. Otolaryngol Head Neck Surg. 2000; 123(3): 334-6.
51. Saydam L, Kizilay A, Kalcioglu T, et al. Ancient cervical vagal neurilemmoma: a case report. Am J Otolaryngol. 2000; 21(1): 61-4
52. Kehagias DT, Bourekas EC, Christoforidis GA. Schwannoma of the Vagus Nerve. American Journal of Roentgenology. 2001;177 (3), 720-1.
53. Leu YS, Chang KC. Extracranial head and neck schwannomas: a review of 8 years experience. Acta Otolaryngol. 2002; 122(4): 435-7.
54. Heasley DC. Case of the month. Schwannoma of the vagus nerve. Crit Rev Comput Tomogr.2003; 44(5): 259-62.
55. Cunningham LL, Warner MR. Schwannoma of the vagus nerve first diagnosed as a parotid tumor. J Oral Maxillofac Surg.2003; 61(1): 141-4.
56. Ford LC, Cruz RM, Rumore GJ, et al. Cervical cystic schwannoma of the vagus nerve: diagnostic and surgical challenge. J Otolaryngol.2003; 32(1): 61-3.
57. Mevio E, Gorini E, Sbrocca M, et al. Unusual cases of cervical nerves schwannomas: phrenic and vagus nerve involvement. Auris Nasus Larynx. 2003; 30(2): 209-213.
58. Rodríguez JCV , Gutiérrez LMJ, Forcelledo MFF, Lucas Villalaín (3), Juan López-Arranz JS. Schwannomas cervicales. Med Oral. 2003;8:71-6
59. Siddiqui BI, Noorni MA, Zaidi SA, Shaiki IA. Peripheral Nerve Sheath Tumor (Schwannoma), arising from an unidentifiable nerve in the neck, with Horner's Syndrome. JPMA (Journal of Pakistan Medical Association). 2003; 53 (5), 1-3.
60. Shetty C, Avinash KR, Auluck A. Schwannoma of vagus nerve masquerating as a parotid tumor. Dentomaxillofac Radiol. 2006; 35(5): 376-9.
61. Szyfter W, Pabiszczak M, Wierzbicka M, Kaczmarek J, Zurawski J. Rare case of the cervical vagal neurinoma. Otolaryngol Pol. 2007;61(5):740-3. doi: 10.1016/S0030-6657(07)70516-4.
62. Kang GC, Soo KC, Lim DT. Extracranial non-vestibular head and neck schwannomas: a ten-year experience. Ann Acad Med Singapore. 2007; Apr;36(4):233-8.
63. Singh D, Pinjala RK. Schwannoma of the cervical vagus nerve. Pediatr Neurosurg. 2007; 43(5): 403-5.
64. Nardello O, Cors A, Pisanu A, et al. A rare case of vagus nerve schwannoma. Chir Ital. 2007; 59(6): 907-10.
65. Matejcik v, Steno J, Haviarova Z, Mvarec B. Neurofibroma of the vagus nerve in the cervical portion. Bratisl Lek Listy. 2008; 109 (10), 455-8.
66. Nakano CG, Massarollo LC, Volpi EM, et al. Ancient schwannoma of the vagus nerve, resection with continuous monitoring of the inferior laryngeal nerve. Braz J Otorhinolaryngol. 2008; 74 (2): 316.
67. Peyvandi A, Samadian M, Ahmady-Roozbahany N. Photoclinic.What is your diagnosis? Photoclinic diagnosis: vagus nerve schwannoma. Arch Iran Med. 2008;11(6):669-71.
68. Chiofalo MG, Longo F, Marone U, et al. Cervical vagal schwannoma. A case report. Acta otorhinolaryngol ital. 2009; 29(1): 33-5.
69. Schupp DJ, Mukherjee D, Sharma GK. Schannoma of the vagus nerve masquerating as a carotid body tumor. Vascular. 2009; 17(4): 2225.
70. Yong DJ, Hailani I, Razif M, Yunus M. Cervical Vagal Schwannoma. Philippine Journal of Otolaryngology Head and Neck Surgery. 2010; 25 (2)- 23-6.
71. Bilancia R, Ampollini L, Cattelini L, et al. Schwannoma of the cervical vagus nerve. Ann Thorac Surg. 2011; 91(1): e13.
72. Lahoti BK, Kaushal M, Garge S, Aggarwal G. Extra vestibular schwannoma: a two year experience. Indian J Otolaryngol Head Neck Surg. 2011;63(4):305-9. Epub 2011 Feb 23.
73. Sreevatsa MR, Srinivasarao RV. Three cases of vagal nerve schwannoma and review of literature. Indian J Otolaryngol Head Neck Surg. 2011;63(4):310-2. Epub 2011 Apr 8.
74. Bergmark RWJ, Guo DP, Lin HW et al. Vagal Schwannoma. Ear, Nose throat J. 2011; 90(9): 410-11.
75. Imperatori, A, Dionigi, G, De Monte L, et al. Cervico-mediastinal schwannoma of the vagus nerve: resection with intraoperative nerve monitoring. Updates Surg. 2011; 63(1): 59-61.
76. Bhandary, K.S., Vaidyanathan, V., Bhat, V., et al. Neck Schwannoma masquerading as a carotid body tumor: Journal of clinical and diagnostic research. 2011; 5(3): 654-6.
77. Gibber, M.J., Zevallos, J.P., Urken, M.L. Enucleation of vagal nerve schwannoma using intraoperative nerve monitoring. Laryngoscope. 2012; 122(4): 790-792.
78. Chiun KC, Tang IP, Prepageran N, Jayalakshmi P. An extensive cervical vagal nerve schwannoma: a case report. Med J Malaysia. 2012; 67(3):342-4.
79. Oyama H, Kito A, Maki H, Hattori K, Noda T, Wada K. Case report schwannoma originating from lower cranial nerves: report of 4 cases. Nagoya J. Med. Sci. 2012;74(1-2):199-206.
80. Chai, C.K., Tang, I.P., Prepageran, N. An extensive cervical vagal nerve schwannoma: a case report. (2012) Med J Malaysia 67 (3): 342-344.
81. Benmansour N, Elfadl Y, Bennani A, Maaroufi M, Chbani L, Amarti A, Tizniti S, Elalami MN. Cervical vagus nerve schwannoma: diagnostic and therapeutic strategies. Pan Afr Med J. 2013; 26;14:76. doi: 10.11604/pamj.2013
82. Gaikwad N, Sathe NU, Wadkar G, Chiplunkar D. Indian J Otolaryngol Head Neck Surg. 2013; 65(Suppl 1):188-91. doi: 10.1007/s12070-011-0475-4. Epub 2012 Jan 6. Schwannoma of the cervical vagus nerve in a child: a case report.
83. Mehta KS, Grupta D, Koul N, Sharm D. Vagal Nerve Schwannoma - A rare neoplasm with a rare presentationa and newer surgical management technique. IOSR Journal of dental and medical sciences. 2013; 9(5):60-5. (IOSR-JDMS) e-ISSN: 2270-0853, p-ISSN: 2279-0861.
84. Simsek G, Sahan M, Gunsoy B, Arirok A, Akin I. Schwannoma of the cervical vagus nerve. A rare benign neurogenic tumor. Otolaryngology online journal. 2013; 3(3): 1-9.
85. Yılmazer R, Yazıcı ZM, Sayın I, Bakan AA, Kayhan FT. Cervical cystic vagal schwannoma mimicking a type 3 second branchial cleft cyst: a case report. Kulak Burun Bogaz Ihtis Derg. 2013;23(3):192-5. doi: 10.5606/kbbihtisas.2013.22448.
86. Bracale U, Sodo M, Strazzullo T, Scotto B, Spera E, Di Salvo E. Cervical vagal schwannoma: single case report. Ann Ital Chir. 2013; 28;84(ePub). pii: S2239253X13021130.
87. Sargar K. Parapharyngeal neck schwannomas with unusual vascular displacement. Case Rep Med. 2013:563019. doi: 10.1155/2013/563019. Epub 2013 Aug 26.
88. Krishnamurthy A, Ramshankar V, Majhi U. Ancient cervical vagal schwannoma: a diagnostic challenge. Indian J Surg Oncol. 2013;4(3):284-6. doi: 10.1007/s13193-013-0245-8. Epub 2013 May 5.
89. Sodhi HB, Salunke P, Sahoo SK. Vagal nerve schwannoma extending from cerebellopontine angle to cervical region straddling across the jugular foramen. Neurol India. 2014;62(2):195-6. doi: 10.4103/0028-3886.132396.
90. Hwang KR, Kim JW, Kim HK, Lee SW. A cervical vagal schwannoma mimicking a parathyroid cyst. Clin Exp Otorhinolaryngol. 2014;7(2):153-6.
91. Agarwal SK, Munjal M, Rai D, Rao S. Malignant Transformation of Vagal Nerve Schwannoma in to Angiosarcoma: A Rare Event. J Surg Tech Case Rep. 2015;7(1):17-9. doi: 10.4103/2006-8808.184941.
92. Tugrul S, Senturk E, Özturan O, Kök A, Buyukpinarbasili N. Schwannoma of the Cervical Vagus with Intrathoracic Extension. J Craniofac Surg. 2015;26(4):e320-2. doi: 10.1097/SCS.0000000000001704.
93. Vijendra SS, Rao RA, Prasad V, Haseena S, Niprupama M. A giant vagal schwannoma with unusual extension from skull base to the mediastinum. J Cancer Res Ther. 2015;11(4):970-3. doi: 10.4103/0973-1482.164697.
94. Kamath PM, Dosemane D, Sreedharan SS, Majeed NA, Shenoy VS. Vagal Schwannoma: A Rare Parapharyngeal Tumour. J Clin Diagn Res. 2016;10(4):MD03-4. doi: 10.7860/JCDR/2016/16391.7588. Epub 2016 Apr 1.
95. McDermott AM, Sadadcharam M, Manning BJ, Sheahan P. Critical Airway Compromise due to a Massive Vagal Schwannoma. Ir Med J. 2016; 10;109(5):408.
96. Abdulla FA, Sasi MP. Schwannomatosis of Cervical Vagus Nerve. Case Rep Surg. 2016:8020919. Epub 2016 Oct 11.
97. Giancarlo DA, Fama I, Morello R, Becelli R. Cervical Vagal Schwannoma Review of all Reported Cases and Our Reports. Int J Neurol Brain Disord. 2016; 3(2): 1- 6.
98. Saini S, Sabharwal N, Agrawal N, Singh B. Cervical Vagal Schwannoma: Anesthetic Concerns. Anesth Essays Res. 2017; 11(1):254-6. doi: 10.4103/0259-1162.183163.
99. Nagavalli S, Yehuda M, McPhaul LW, Gianoukakis AG. A Cervical Schwannoma Masquerading as a Thyroid Nodule. Eur Thyroid J. 2017;6(4):216-20. doi: 10.1159/000454877. Epub 2017 Jan 21.
100. Carroll C, Jagatiya M, Kamel D, Siddiqi J. A parapharyngeal space schwannoma arising from the vagus nerve: A case report. Int J Surg Case Rep. 2017;41:22-5. doi: 10.1016/j.ijscr.2017.09.025. Epub 2017 Oct 5.
101. Ansari I, Ansari A, Graison AA, Patil AJ, Joshi H. Head and Neck Schwannomas: A Surgical Challenge-A Series of 5 Cases. Case Rep Otolaryngol. 2018; 4;2018:4074905. doi: 10.1155/2018/4074905. eCollection 2018.
102. Kumar P, Alam S. “Collateral Damage:” Horner's Syndrome Following Excision of a Cervical Vagal Schwannoma. Int J Appl Basic Med Res. 2018; 8(3): 190–192.doi: 10.4103/ijabmr.IJABMR_439_16
103. Mierzwiński J, Wrukowska I, Tyra J, Paczkowski D, Szcześniak T, Haber K. Diagnosis and management of pediatric cervical vagal schwannoma. Int J Pediatr Otorhinolaryngol. 2018;114:9-14. doi: 10.1016/j.ijporl.2018.08.021. Epub 2018 Aug 23
104. Cukic O, Jovanovic MB. Vagus Nerve Schwannoma Mimicking a Lateral Neck Cyst. J Craniofac Surg. 2018;29(8):e827-e828. doi: 10.1097/SCS.0000000000005006.
105. Mat Lazim N. Challenges in managing a vagal schwannomas: Lesson learnt. Int J Surg Case Rep. 2018;53:5-8. doi: 10.1016/j.ijscr.2018.10.025. Epub 2018 Oct 19.
106. Kumar KP, Alam MS. "Collateral Damage:" Horner's Syndrome Following Excision of a Cervical Vagal Schwannoma. Int J Appl Basic Med Res. 2018;8(3):190-192. doi: 10.4103/ijabmr.IJABMR_439_16.
107. Dindigal RN, Maramreddy R, Bhat S, Shetty SK. Cervical Vagal Schwannoma: Peculiarity in Diagnosis and Treatment. Journal of Clinical and Diagn Res. 2018; 12(5): 20-1. doi:10.7860/JCDR/2018/33983.11531
108. Bhattacharya K, Sarkar SD, Biswas T. Case Report Vagal nerve schwannoma: a rare case from Border Security Force Composite hospital. International Surgery Journal Bhattacharya K et al. Int Surg J. 2019;6(1):307-9 http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902.
109. Anil G, Tan TY. Imaging characteristics of schwannoma of the cervical sympathetic chain: a review of 12 cases. AJNR Am J Neuroradiol 2010;31:1408-12.
110. Colreavy MP, Lacy PD, Hughes J, Bouchier-Hayes D, Brennan P, O'Dwyer AJ, Donnelly MJ, Gaffney R, Maguire A, O'Dwyer TP, Timon CV, Walsh MA. Head and neck schwannomas--a 10 year review.J Laryngol Otol. 2000; 114(2):119-24.
111. Nao EEM, Dassonville O, Bozec A, Sudaka A , Marcy PY, Vincent N, Pierre S, Riss JC, Fakhry N, Santini J, Poissonnet G.Cervical sympathetic chain schwannoma European Annals of Otorhinolaryngology, Head and Neck diseases. 2012; 129, e51-e53