
Experience with Burn Prevention Program in North Eastern India
Main Article Content
Abstract
Burn injuries are one of the most devastating of all injuries and a major global public health concern. Though burn injuries cause lots of morbidity and mortality in India, community-based interventions in the forms of multi-strategic and multi-focused preventive programs are however lacking. This study, undertaken in the North Eastern Indian state of Assam, aims at reducing the incidence of burn accidents, morbidity and mortality of burn injuries through focused attention towards sensitizing the community with well-structured preventive program.
Participatory community seminars, use of print, electronic and social media and lectures and demonstrations in schools were the tools used in the preventive programs.
Analysis of inpatient and outpatient records of burn injured patients treated in the burn unit and scoring system in school education program and social media participants helped in assessment of the impact of Burn Preventive Programs (BPP). For convenience of assessment, comparative analysis of the results in early (Block I) and later part (Block II) of the study period was made.
Results showed significant reduction of percentage of patients reporting from the areas where BPP was implemented. There was also reduction in %TBSA burn in majority patients in Block II in comparison to Block I. Water was used to extinguish fire in 48.9% patients in Block I and 78.0% patients in Block II. Water was also used to cool burn wounds by 52.3% patients in Block I, and 83.4% patients in Block II. While 80.9% people made inappropriate topical application on the wounds in Block I, only 34.6% did so in Block II. Increased awareness amongst general people was reflected by increased percentage of patients reporting to burn unit within 7 hours of injury and significant reduction of firecracker burns from 21.9% (Block I) to 7.8% (Block II). Similarly, improved awareness amongst the students was evident from the improved scoring by majority students and reduction in burns amongst them in the later part of Block II. The results indicate that BPP has got positive impact in the society.

1 . Introduction
Burn injuries are one of the most devastating of all injuries and a major global public health concern [1, 2] . Approximately 90 percent of burns occur in low and middle - income countries, regions that generally lack the necessary infrastructure to reduce the incidence and s everity of burns . [3, 4] However, reduction in preventable burn deaths can be achieved by investment in safe living conditions and equitable access to medical care.
Estimates of incidence of burn injuries in India are most likely to be informed guesses. J . W. L. Davis [ 5 ] quoted an incidence of two million burn injuries annually; 0.5 million of them receive clinic or hospital outpatient care, 0.2 million are admitted to hospitals and 50000 succumb to the injuries. The figures quoted may be a gross undere stimation as numerous burn injuries, especially from rural population remain unreported. According to the data published by National Health portal of India (Last updated in 2016) ( https://www. nhp.gov.in/disease/skin/burns #: ) 7 million people suffer from burn injuries every year with 1.4 lakhs (0.14 million) death and 2.4 lakh s (0.24 million) suffering from various disabilities. 75% of the burn injuries occur at home and 80% of the victims are the women and children [ 6 ]. In recent years, increase in the number of terrorist violence, bus, train and airplane accidents, fire in the high - rise buildings and industrial accidents have all contributed to the swelling in the number of casualties of burns [ 7 ] .
Inadequate treatment facilities in the country as a whole, compounded by ignorance, superstition and misconception prevailing in the community in general , have made the burns management far from adequate. About 60 existing burn units, mostly located in the major cities of the country, are grossly insufficient to provide burn care to the large number of burn injured patients [ 8 ]. The scenario in the North East India, consisting of seven states (where this study was done) is still worse. A large number of patients of this region are still deprived of proper care because of the poor facilities for burn care in the government and private institutions.
Burn injuries are therefore better prevented than treated. There are encouraging reports of reduction of incidence and mortality of burns in developed countries due to effective implementation of Burn Prevention Program [ 9, 10 ]. The author published a study on the positive impact of Burn Prevention Program (BPP) on the community as a whole in respect of Fir st Aid and Prevention of burn accidents [ 11 ] . This study was conducted in two hospitals in the state of Assam, namely Indian Oil Corporation (Assam Oil Division) Hospital, Digboi and Guwahati Refinery Hospital , in a period of 13 years (1994 to 2007). Subse quently, t he BPP was continued through the Burn Unit of Burn Care Foundation, in the city of Guwahati ( the capital city of Assam ) , with addition of more prevention tools. In the COVID 19 pandemic year (2020), due to loss of social contact amongst the peop le, BPP had to be carried out digitally and through social media. BPP was implemented with some changed concept, namely , Primary, Secondary and Tertiary Prevention Program, aimed at reduction of incidence through education of people , reduction of severity by proper use of first aid measures and reduction of complications of burns by appropriate tertiary care.
The Burn Unit of Burn Care Foundation, a trust of NEMCARE Hospital, Guwahati, is a 10 bedded tertiary B urn C are U nit, catering to the needs of the sev en North – Eastern states of India. This unit, equipped with ICU beds, operation theatre and all modern burn care equipments , is manned by a dedicated and trained burn care team . Use of advanced burn management protocols in the burn unit, like proper fluid r esuscitation, use of modern burn wound covers and routine use of Early Excision and Skin Grafting in full thickness burns, have improved morbidity and mortality of burn patients. P atients with majors burns , referred from different neighboring states and th ose from the state of Assam and the city of Guwahati are the beneficiaries of the b urn unit. There being other hospitals in the city, which treat burn injured patients, the number of patients treated in this unit do not represent the incidence of burns in the region.
The Burn unit is also engaged in Burn Prevention Programs like - Public Awareness P rograms, School Education Programs, e rection of hoardings (with writings on First aid and Prevention of Burns) at public places, publication of articles in news pa pers and journals , T alks and Interviews o n television and T alks and W ritings in Social M edia. Most of the tools of Burn Prevention were being used by the author since 1994 , with addition of Annual Burn Care Day and use of social media in recent past. The b urn u nit also organize d Training Programs for doctors , nurses and paramedics on Essential Burn Care in the entire North East India to boost up the burn care in the region.
The present study was the analysis of the records of the BPP undertaken by the B urn U nit of Burn Care Foundation, aiming at ascertaining the impact of the program on the community as a whole. The inpatient records of the burn unit and the records of school education and public awareness program s from 2010 to 20 20 (1 0 years) were analyzed. These records of the two periods - namely 2010 to 2015 (Block I) and 2016 to 2020 (Block II) were com p ared to have a feed back on improved impact of the program on the society.
2. Materials and Methods
A data base was created on the admitted patient s as regards to their nature of injury, circumstances leading to the injuries, the social, educational and economic status of the patients, nature of first aids received, treatment modalities and the results of treatment received. The records of each patie nt were collected from the format used by Burn Unit and later on from format provided by WHO for World Burn Registry. These formats were filled up by doctors and nurses while the patient s were undergoing treatment in the burn unit. The records of the patie nts treated in Out Patient Department (OPD) were collected from the filled - up formats used in the burn unit.
The structured preventive programs of the present study were designed to cover 3 million population of the city of Guwahati only. As the awareness level on burns of the targeted people was low and the incidence of burns was high among st all groups, the prevention program was designed to cover topics on general awareness on the subject.
The study was approved by the hospital ethical committee.
The tools for prevention program used are described below:
2 .1 . Seminars and discussions
Participatory community sessions were organized at public places in the entire city of Guwahati. A total of 35 such sessions were organized. Adult males and females f rom all socio - economic status participated. Following topics were discussed by audio - visual means in those sessions.
a. Causation, types and first aid in burns, with emphasis on use of water for extinguishing fire and cooling the burn wounds.
b. Avoidance of any topical application on burn wounds as first aid .
c. Preventive measures to be adopted in the kitchen, other places at home and in the industry to prevent fire accidents.
d. Identification of hazards of fire and burn accidents that looms large at household and a t workplace.
e. Importance of early reporting to hospital after occurrence of burn injuries.
2 . 2. School Education Program
A total of 70 schools were included in the program. Thirty - five schools were covered in each Block. Two programs were conducted in eac h school annually at a gap of six months. The participating students were from VIII, IX and X standards. Audio - visual presentations on various aspects of burns were the main tool of prevention p rogram in all the schools covering 4200 students in both the Blocks. Seventeen schools in each Block were also provided with reading materials on burns on first visit. Eighteen schools in each block received only audio - visual presentation. The students of these schools did not receive reading materials.
Students at each school were provided with written questionnaire, containing ten questions (Appendix I) , to be answered immediately, on the second visit . They were also given five tasks on burn prevention for implementation at home (appendix II). The questionnaire had 10 scores and the tasks on preventive measures had 10 scores. These were evaluated on the basis of performance of the participating students.
2.3. Publication of articles
Articles on First Aids and Prevention of Burns were published in the house Journal s , periodicals and newspapers.
2.4. Display of banners and posters – Banners and posters containing messages on First Aid and P revention of Burns were displayed at public places.
The following tools were added in the preventive programs in later part of B lock I.
2.5. Special preventive program before Diwali
Diwali, a popular festival of light is celebrated by lighting earthen lamps and candles and bursting fire crackers . Burn injuries of hands and faces are of common occurrences every year due to carele ss handling of fire crackers during the festival. Special BPP were arranged three weeks preceding the festival to educate the people on safe handling of fire and crackers. The program included one common school education program inviting students of 7 - 8 sc hools in a large auditorium , one community session annually (in addition to the routine annual program of prevention), display of posters and banners and distribution of special booklets and greeting cards, containing dos and don’ts in Diwali. From 2019 on wards, we started the slogan - “Say ‘no’ to fireworks in Diwali ” . On our special appeal, t he local administration of each district, en acted l egislation to limit the time and place of fireworks during the festival, which helped in reduction of burn accidents .
2.6. Publication of books and booklets
A book on burn injuries , written in local l anguage and two booklets, written in English and Assamese were distribut ed amongst the students and common people.
2.7. Interactions with the electronic and print media
This was done by arranging press meet every year before the festival of Diwali.
2.8. Talks on television channels
Minimum three talks on Burn Prevention were arranged in television channels every year.
2.9. Burn Care Day
Since 2015, a daylong participato ry community program involving the doctors, nurses, paramedics, hospital administrators, students and common people were organized. This annual event was aimed at making the people, including medical professionals aware of Burn Prevention and also the prob lems faced by burn injured patients. Audio - visual talks on F ir st A id and P reventi on of B urn A ccidents were arranged for the participants. Illustrative talk on newer modalities of treatment and their positive effects on all types of burn s was another tool o f public awareness , used. A leading journalist and a celebrity like a film star were invited to the session for better publicity of the event.
2.10. Use of Social media
In the COVID 19 affected year (2020 ), with no community gathering, BPP was continued through social media like Face book and You Tube. Access to internet and social media by youth being higher , we use d these media to spread the message of b urn p revention and also to collect feedback. Three talks , with illustrations , on Causation, First A i d and Prevention of Burns were uploaded in Face B ook and You T ube. A questionnaire containing 10 short questions (Appendix III) was also uploaded after one month. The feedback received through comments and messenger was recorded.
Two Webinars were also or ganized in that year to make people aware on burn prevention before the festival of Diwali .
Impact of BPP was assessed by analyzing the data obtained from the records of patients treated in the burn unit and from the score s of the students and participants in BPP . T he relevant data were collected from the computerized inpatient and outpatient records, which were regularly updated from the formats used to collect data from the patient and the attendants at the time of reporting to hospital and th ereafter. Since 2015, we started using the format of World Burn Registry, supplied by WHO . These formats contained the histories with special reference to date and time of occurrence of burn accident, causative factors of burns, types of clothing worn at t he time of incidence, education and social status of the patients and the nature of first aid received at the site of injury. Collected data also included number of inpatients and outpatients, their age and sex and percentage of burns, treatment received and follow ups .
2.11. Data analysis
Data was entered and analyzed in SPSS software version 25 .0 for windows. For difference in categorical variables, Pearson Chi square χ2 test was used. A value of P<0.0 5 was considered statistically significant. For da ta analysis mean and SD were used as descriptive statistics.
3. Results
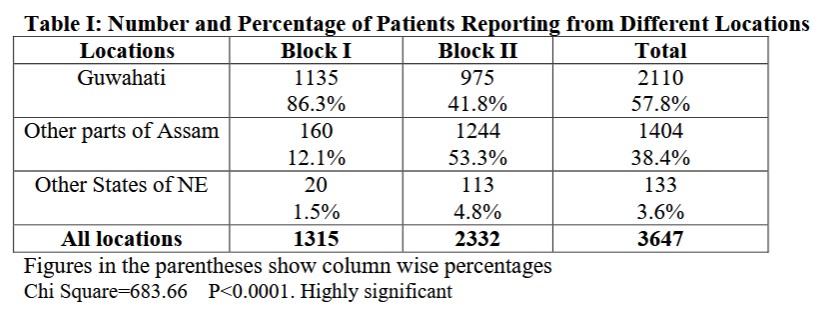
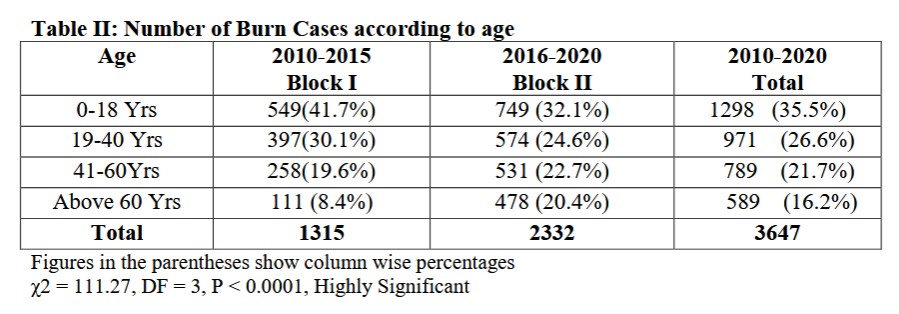
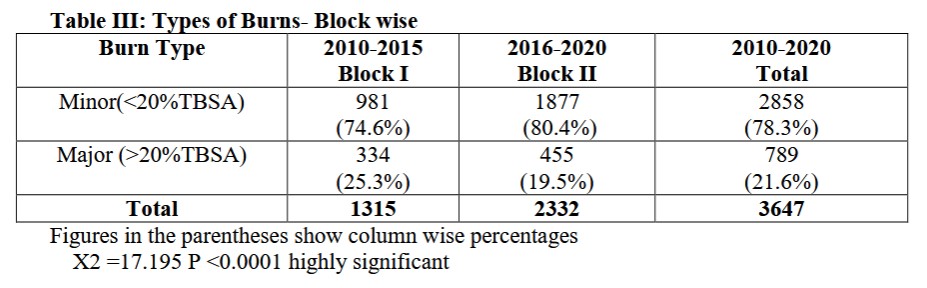
A total of 3647 patients were treated in the Burn Unit from October 2010 to October 2020 ( 10 years); 1270 as inpatients and 2377 as out patients. 3514 (96.3 %) patients were from Assam . while 133 ( 3.6% ) were from other North - Eastern states . Patients from Assam included 2110 (57.8%) numbers from the city of Guwahati and 1404 (38.4%) from other parts of Assam (Table I) . There were 204 7 males and 1600 female patients. 1298 ( 35.5 %) patients were below 18 years , 971 ( 26.6 %) were between 19 – 40 Years of age. Data also indicated that there were 28 58 (78. 3 %) numbers of minor burns (<20%TBSA) and 7 89 ( 21. 6 %) numbers of major burns in the study . M ajor Burns ( > 20% TBSA ) were commonly seen among st t he young people (19 - 40 years); t hey were less common in children and elderly. ( χ2 = 402.51, DF = 9, P < 0.0001, Highly Significant) ( Fig I ). Analysis also revealed that there was significant reduction o f burns ( χ2 = 111.27, DF = 3, P < 0.0001 ) in children (1 - 18yrs) and young adults (19 - 40yrs) in Block II ( Table I I ) . Data analysis als o revealed that percentage of major burns was significantly reduce d ( X2 =17. 195 P <0.0001 ) in Block II in comparison to Block I. (Table I II )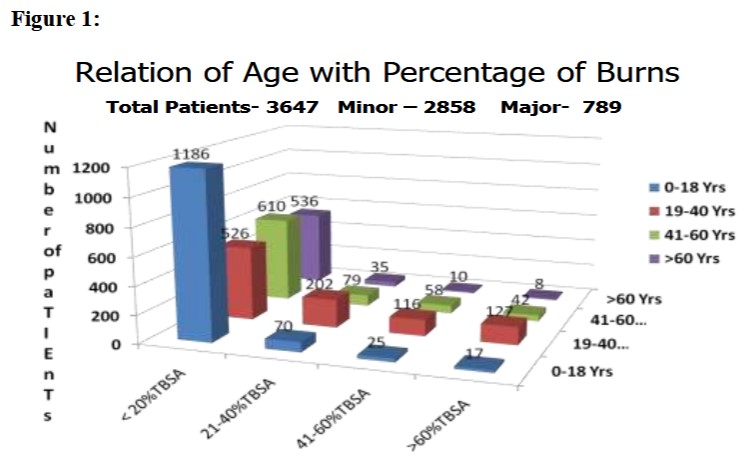
χ2 = 402.51, DF = 9, P < 0.0001, Highly Significant
3.1. Number of patients reporting to burn unit
A total of 1315 patients reported to the burn unit for treatment in Block I; 389 were treated as inpatients and 926 as outpatients. In Block II, out of 23 32 patients reporting for treatment, 881 were inpatients and 1451 as outpatients. The increased number of patients reporting to Burn unit in Block II could be attributed to increased number of referrals from different medical facilities, as more people cam e to know about the improved burn care of the tertiary burn care unit. This increase cannot be linked to the incidence of burns in the region. But, on analyzing the locations of the patients, from where they reported for treatment, it was found that there was significant reduction of percentage of patients in Block II (Chi Square=683.66 P<0.0001) (86.3% in Block I and 41,8% in Block II) from the city of Guwahati, where the Prevention Program was primarily implemented (Table I).
3.2. Methods used to extinguish fire Out of 1315 patients, who reported to the burn unit in Block I, 644 ( 48.9% ) poured water, 3 95 ( 30.0 %) used blanket and 158 ( 12.0 %) rolled on the ground to extinguish fire. Rest 15 (2.2%) patients ran out of fear and sustained major burns. In Block II, out of 2332 patients, a significantly increased number ( P < 0.0001 ) i.e., 1819 ( 78.0 %) poured water to extinguish fire, 140 ( 6.0 %) used blankets (significant decrease P < 0.0001 ) , 233 ( 10.0 %) rolled on the ground and rest 140(6.0%) patients ran shouting for help, and thereby courting major burns (Table I V ).
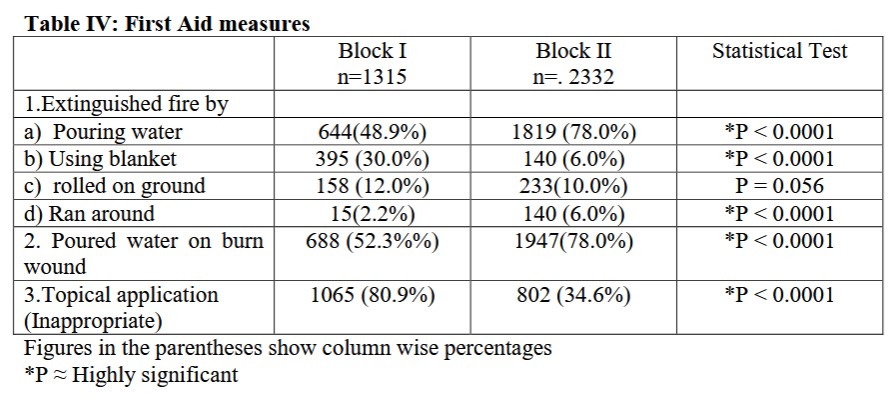
3.3. First aid measures
688 ( 52.3% %) patients poured water to cool the burn wounds in Block I; while a significantly increased number of patients - 1947 (7 8 .0%) did so in Block I I (P < 0.0001) . 16 0 patients ( 6.8 %) with minor burns of the limbs repor ted to the burn unit with their burnt limbs submerged in bucket full of water , indicating better awareness on first aids. Inappropriate topical applications , like toothpaste, egg yolk, ghee, boiled and mashed potato, grease, ashes etc. over the burn wound as first aid , were noted in 1065 patients (80 .9 % ) in Block I. But the number of people resorting to inappropriate applications came down significantly (P < 0.0001 ) to 802 ( 34. 6 %) in Block II ( Table I V ).
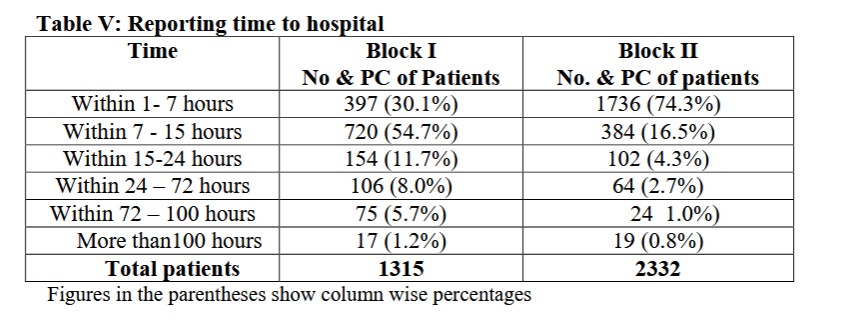
3.4 Reporting time in hospital
Analysis of the repo rting time to hospital revealed that 397 (30.1%) patients reported within 7 hours in Block I, as against 1737 (74.3%) patients reporting within 7 hours in Block II. It was also evident that 90.8 % patients reported to burn unit within 15 hours in Block II a nd 84.4% reported within the same time in Block I (Table V).
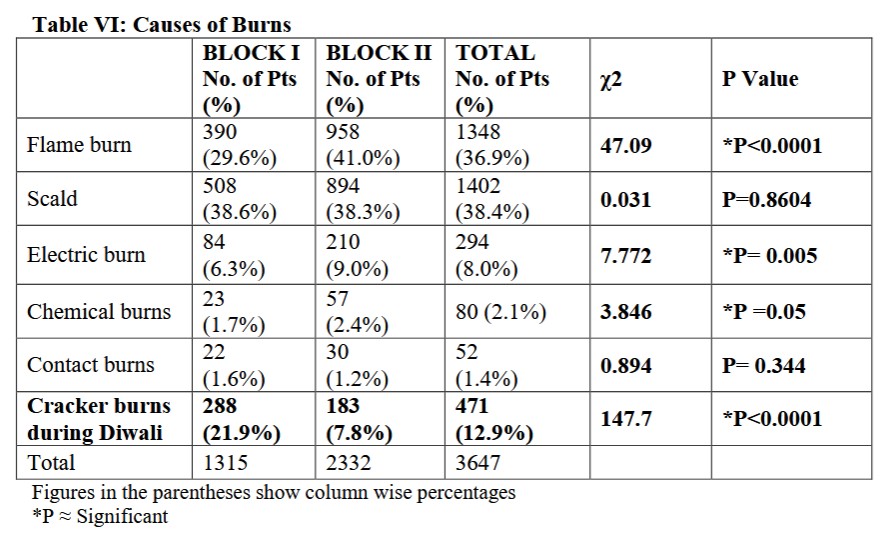
3.5 Caus es of burns
While analyzing the agents causing burns , it was revealed that the number of burn injuries caused by other agents remaining almost at par in two blocks, there was significant reduction (P < 0.0001 ) in the burns caused by firecracker injury in Block II in comparison to Block I (Table V I )
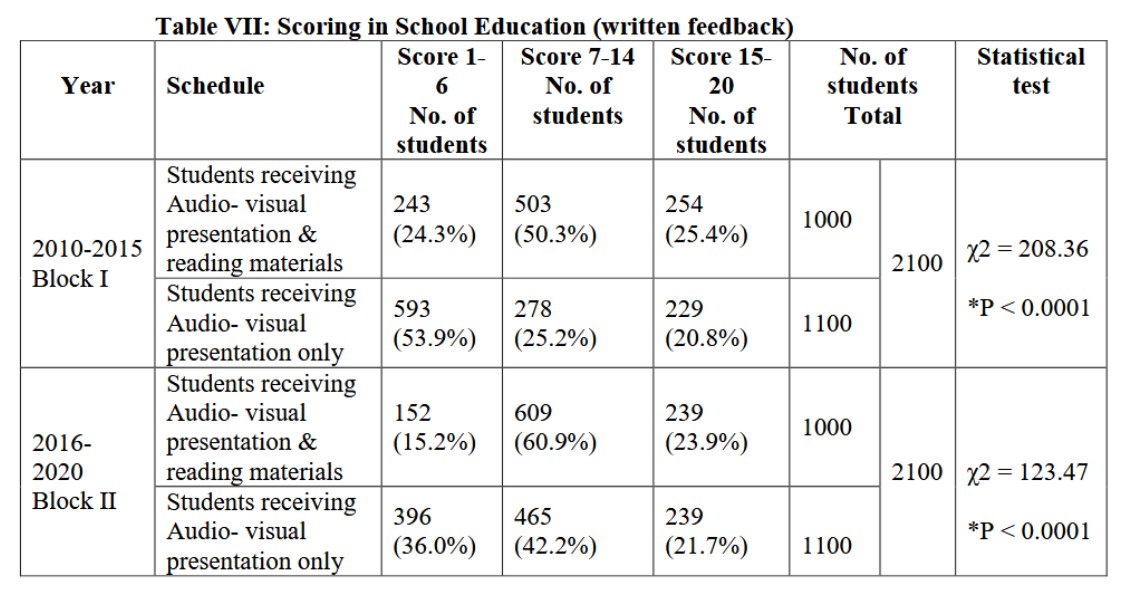
3.6 School Educat ion Program
A total of 4200 students of 70 schools participated in the School Education Program organized in two blocks. All students took part in feedback by filling up the written Questionnaire introduced in both the Block s . S cores of students of two gr oups were compared for better assessment of impact of education. Results revealed moderate , but significant improvement in scores of the students, who were provided with reading materials along with audio - visual presentations . T he students , who were not gi ven any reading material, did not recall the presentations so well as compared to the other group (Table VII ).
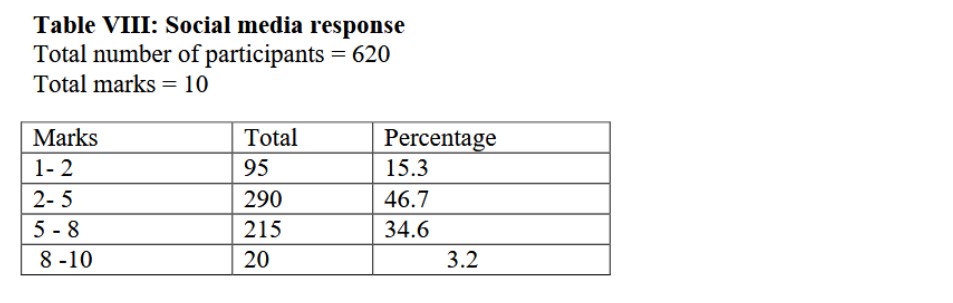
3.7 Use of Social Media
A total of 620 people responded to the questionnaire, u ploaded in Facebook. Majority of them could recall and score d good marks. O ut of 10 marks, 95 (15.3%) participants got 1 - 2 marks, 290 (46.7%) participants got 2 - 5 marks, 215 (34.6%) got 5 - 8 marks and 2 0 (3.2%) of them scored between 8 - 10 marks (Table V III ).
4 Discussion
Non availability of accurate data on incidence of burns in India seriously limits planning for burn s manag ement and preventive strategies. Inadequate treatment facilities have deprived many deserving patient ’ s access to proper management [ 8 ] . The cost of burn care is formidable. The patients are mostly from poor socio - economic status. Majority of the patients end up with severe morbidity or mortality [ 9 ] Amongst those who survive, a major burn injured patient (above 20% TBSA) takes at least a month or two to be fit enough to leave the hospital He/she takes another three to four months to resume his /her normal work [ 6 ]
The tertiary Burn Care Unit (where the present study was done) with modern burn care facilities , cater ed to the need of all referred cases from primary and secondary care units of the entire North Eastern States. But, as there were other governmen t and private facilities located in the city, many patients were treated in those facilities as well. Hence the patient reporting to the unit , did not represent the incidence of burns in the locality. However, analysis of the data revealed that there was a definite reduction of percentage of patients reporting from the city of Guwahati to the Burn Unit in the Block II, indicating that Burn Prevention Program undertaken in the city had positive impact. Reduction of number of burn injuries amongst the childre n and young adults in Block II was another indication of positive impact of School Education Programs in our study. These results also corroborate with the findings of the earlier study of the author, where the patients reporting to the burn unit from a pa rticular captive locality , showed significant reduction of average admission per year in the Block II after community based BPP [ 1 0 ] . Similar reduction of admission of burn injured children after community - based intervention program was also shown in an in jury prevention study [ 1 1 ] . Two out of four included studies in a Cochrane review reported a significant decrease in pediatric burn and scald injury in the intervention compared with the controlled community [ 12 ] . Another community - based intervention study showed that due to regionalization of burn care and intensification of fire prevention initiatives, there was reduction in incidence of death and hospitalization resulting from burns [ 13 ] .
The effectiveness of the BPP was also ascertained by use of first aid measures like pouring of water on burn wounds, avoidance of application of topical agents as first aid measure and decrease in number of fire cracker burns during Diwali. Reduction of percentage of major burns in Block II in comparison to Block I in th e present study indicate d better awareness on methods of extinguishing fire and better f irst aid measures . A study of first aid and initial management for childhood burns in Vietnam revealed that cooling of the burn wound surf ace by cold water was applied only in 27.17% of their cases. The authors recommended public education on first aid measures to improve compliance [ 1 4 ] . The present study which showed improved compliance to cooling of burn wounds by application of cold water , after community participat ive education program , was in agreement with these recommendations. The significant reduction of percentage of major burns in Block II, in comparison to Block I in our study, can also be attributed to increased number of people resorting to cooling of the burn wounds .
As many patients, especially from rural area s wasted time b y resorting to unconventional treatment and application of herbal medicines, before coming to the hospital [1 5 ] , we had difficulty in resuscitating them. Repeated messages o n importanc e of early reporting to hospita l given through prevention program in our study, improved compliance. This was evident from increased percentage of patients reporting to burn unit within 7 hours in Block II in comparison to Block I.
The task of educating st udents was easier as they were found to be more receptive and were known to spread the messages to their parents and friends. This fact was corroborated by the study done by M. H. Keswani in the schools of Bombay . H e documented that students exposed to BPP could recall the imparted knowledge on questioning without hesitation; but it was not the case with those students who were not exposed to such program [ 16] . Our study also revealed better awareness and better scoring by students getting education - both a udio - visual presentation and reading materials, than those, who were given only audio - visual presentation in both the blocks. B etter scoring by the students even without getting reading materials in Block II could be attributed to their exposure to televis ion talks and social media presentation in the later part of the study. Many students transmitted the information to their parents and friends as well. One of the studies, where follow up was done in a school - based scald prevention program , the authors sho wed that students could recall 7.6 out of 10 scald hazards, told to them. In the same study , 65 - 70% children reported the use of the safety items shown to them , in their residence , for a variable period of time [ 1 7 ] . Our results also showed significant re duction of burns amongst school going children in the later period of Block II, indicating positive impact of education. I n another study, where evaluation of prevention program of scald and burn injury in young children was done , the parents and guardians of the exposed children were found to be 1.5 – 5 times more aware of the prevention message than those not exposed to the program [1 8 ] . In another study, the authors found that, in localities with burn prevention programs, there was a reduction in the rat e of burn - related hospitalizations of infants, from 1.39 to 1.05 per 1000 infants (p<0.05), in contrast to localities where programs did not exist. The greatest change was in middle and high socio - economic communities. The prevention programs had no simila r effects on school - aged children. They concluded that injury prevention programs are effective in reducing burn - related hospitalizations among infants and toddlers, especially from more affluent communities, but not among school - aged children [1 9 ]
Our attempt at using social media as a tool burn prevention in the COVID 19 affected year , showed encouraging result, as majority of the participants could reply to our short questionnaires even after a month of uploading the presentation on Burns. This could be an effective tool of burn prevention, as a sizeable number of people now use social media. Our inference has been corroborated by a study in a school in Bangladesh which showed that the students had previous knowledge of First aid and prevention of burns, as 32% of them had regular and 45.3% had sometimes access to internet [ 2 0 ] . The decrease d incidence of firecracker burns during Diwali in Block II of our study indicated that burn prevention messages transmitted by special campaign just before the Diwali , along with the strict legislation, limiting playing with firecrackers by the district administration, did percolate to the targeted masses. Our findings were corroborated by a study on Diwali Burns, which commented that “All over the world incidence of bur n injuries due to firecrackers continues to fall due to proper legislation, strict implementation and increasing public awareness” [ 21,22,23,24].
4.1 Future prospect of study
The present Prevention Program is an other attempt to make people aware on Burn Prevention Module in a thickly populated city. There is every scope to make the program more scheduled to cover the targeted people in more systematic way. Our study revealed that a particular group of people - namely electrical workers sustain ghastly burn injuries with high mortality and morbidity. Lack of awareness on burn injury prevention being the primary cause, a structured preventive program with hazard identification and mitigation may prove useful for them. The comparison of information acquired and retained by the workers who a re exposed to BPP with those not exposed (Control), will be a better proposition for judging the effectiveness of the program. In a study of school - based scald prevention program, the authors documented that those children who received the program , showed considerable improvement in hazard identification at the post test, while children in the controlled school showed minimal improvement [ 2 5 ] .
The present program has been able to make some impact on the targeted people in a pos itive direction. It can now be the basis upon which further improvement on the program can be made.
5 Conclusion
Burn Prevention Program aimed at educating the people a nd the students in a thickly populated city , has served the purpose to a certain extent . The impact of BPP was evident from significant lowering of percentage of patients reporting from the targeted location and incidence of firecracker burns during Diwali. Students participating in the school education program showed better awareness as was evident from decrease number and in severity of burns amongst them and from better recall of the preventive measures on questioning . Use of social media as a tool of Burn prevention has also shown promising result. It can be concluded that community - based preventive program can reduce burn injuries and severity of burns.
Acknowledgement -
The authors are thankful to the Management of NEMCARE Hospital, Guwahati for providing the help and support necessary for carrying out the prevention program and also for allowing publishing the results. Our sincere thanks are also due to the staff and colleagues of the Burn Unit of NEMCARE Hospital for their active participation in the program.
Article Details
The Medical Research Archives grants authors the right to publish and reproduce the unrevised contribution in whole or in part at any time and in any form for any scholarly non-commercial purpose with the condition that all publications of the contribution include a full citation to the journal as published by the Medical Research Archives.
References
[2] Peck MD, Kruger GE, Vander Merwe AE, Godakumbura W, Ahuja RB: Burns and fires from non-electric domestic appliances in low- and middle-income countries Part I. The scope of the problem. Burns. 2008 May; 34(3):303-11.
[3] Murray CJL, Lopez AD: The Global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. World Health Organization, World Bank & Harvard School of Public Health. (1996). https://apps.who.int/iris/handle/10665/41864
[4] Peck M, Pressman MA: The correlation between burn mortality rates from fire and flame and economic status of countries. Burns. 2013 Sep; 39(6):1054-9.
[5] Davies JW. The problems of burns in India. Burns. Burns Suppl 1990;1: S4-24.
[6] Keswani MH. In: Hanumadass M and Ramakrishnan M, editors History of Burn Care and Burn prevention Program in India- Handbook of Burns Management-. Jaypee Brothers Medical Publishers Private Limited;1991
[7] Gupta JL. In: Hanumadass M and Ramakrishnan M, editors Planning a Burns unit- Handbook of Burns Management- Jaypee Brothers Medical Publishers Private Limited;1991
[8] Gupta JL. History of Burn Care in India. Indian J Burns. 2005(December):13 -01.
[9] Olaitan PB, Olaitan JO. Burns and scalds--epidemiology and prevention in a developing country. Niger J Med. 2005 Jan-Mar;14(1):9-16.
[10] Sarma BP. Prevention of burns: 13 years' experience in Northeastern India. Burns. 2011 Mar;37(2):265-72.
[11] Ytterstad B, Smith GS, Coggan- Harstad CA. Injury prevention study: prevention of burns in young children by community-based intervention. Inj Prev. 1998;4(3):176-180
[12] Turner C, Spinks A, McClure RJ, Nixon J. Community-based interventions for the prevention of burns and scalds in children. Cochrane Database Syst Rev. 2004; doi: 10.1002/14651858.CD004335.pub2.Issue Art. No:CD004335.
[13] Clark DE, Dainiak CN, Reeder S. Decreasing incidence of burn injury in a rural state. Inj Prev. 2000 Dec;6(4):259-262. doi: 10.1136/ip.6.4.259-a.
[14] Lam N, Dung N. First aid and initial management for childhood burns in Vietnam--an appeal for public and continuing medical education. Burns. 2009 Feb;34(1):67-70.
[15] Shanmugakrishnan RR, Narayanan V, Thirumalaikolundu subramanian P. Epidemiology of burns in a teaching hospital in south India. Indian J Plast Surg. 2008; 41(1):34-37.
[16] Keswani MH. The prevention of burning injury. Burns. 1986. 12 (8) 533-539.
[17] Moore J, Morath K, Harré N. Follow-up study of a school-based scalds prevention programme. Health Education Research. 2004 Vol.19 Oxford University Press. p 430-439.
[18] Macarthur C. Evaluation of Safe Kids Week 2001: prevention of scald and burn injuries in young children. Inj Prev. 2003 Jun;9(2):112-116.
[19] Peleg K, Goldman S, Sikron F. Burn prevention programs for children: do they reduce burn-related hospitalizations? Burns. 2005 May;31(3):347-50.
[20] Arifuzzaman M, Muhammad F, Farahnaz S, Chowdury ARMM, Shahjahan M, ChowdhuryABMA. Burn Prevention and First Aid knowledge among high school students in Bangladesh. Daffodil International University Journal of Allied Health Sciences. 2016 3(1) 41-49. http://hdl.handle.net/20.500.11948/1881
[21] Upadhyaya DN, Khanna V: Diwali Burn; An Overview.2012, Indian J Burns. 20.(1) 46-47
[22] Johnston JJ, Jenkins M, McKinney LA: Fireworks related injuries: Does changing legislation make a difference? A thought for next Halloween. Emerg Med J 2001; 18:232.
[23] Fogarty BJ, Gordon DJ: Firework related injury and legislation: The epidemiology of firework injuries and the effect of legislation in Northern Ireland. Burns 1999; 25:53-6.
[24] D'Argenio P, Cafaro L, Santonastasi F, Taggi F, Binkin N. Capodanno Senza Danno: The effects of an intervention program on firework injuries in Naples. Am J Public Health 1996; 86:84-6.
[25] Harré N, Coveney A. School-based scald prevention: reaching children and their families. Health education research theory and practice. 2000 Apr;15(2):191-202.